Lung cancer is the leading cause of cancer morbidity and mortality worldwide. Apart from tobacco smoke and dietary factors, microbial infections have been reported as the third leading cause of cancers globally. Deciphering the association between microbiome and lung cancer will provide potential biomarkers and novel insight in lung cancer progression. In this current study, we performed a meta-analysis to decipher the possible association between C. pneumoniae and human papillomavirus (HPV) and the risk of lung cancer.
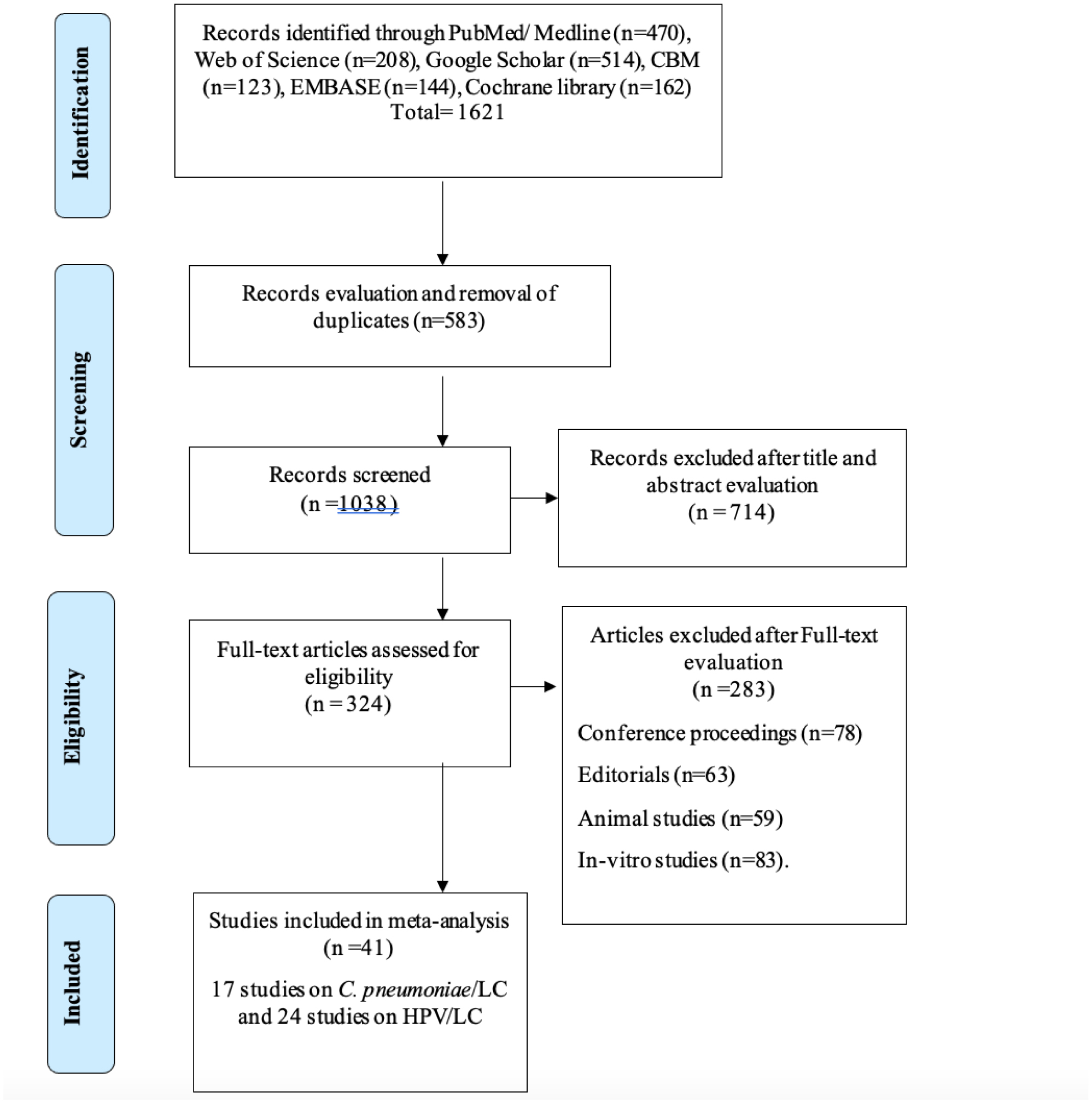
Literature search was conducted in most English and Chinese databases. Data were analyzed using CMA v.3.0 and RevMan v.5.3 software (Cochrane-Mantel-Haenszel method) by random-effects (DerSimonian and Laird) model.
The overall pooled estimates for HPV studies revealed that HPV infections in patients with lung cancer were significantly higher than those in the control group (OR = 2.33, 95% CI = 1.57–3.37, p < 0.001). Base on subgroup analysis, HPV infection rate was significantly higher in Asians (OR = 6.38, 95% CI = 2.33–17.46, p < 0.001), in tissues (OR = 5.04, 95% CI = 2.27–11.19, p < 0.001) and blood samples (OR = 1.40, 95% CI = 1.02–1.93, p = 0.04) of lung cancer patients but non-significantly lower in males (OR = 0.84, 95% CI = 0.57–1.22, p =0.35) and among lung cancer patients at clinical stage I-II (OR = 0.95, 95% CI = 0.61–1.49, p = 0.82). The overall pooled estimates from C. pneumoniae studies revealed that C. pneumoniae infection is a risk factor among lung cancer patients who are IgA seropositive (OR = 1.88, 95% CI = 1.30–2.70, p < 0.001) and IgG seropositive (OR = 1.50, 95% CI = 1.10–2.04, p = 0.010). All seronegative IgA (OR = 0.69, 95% CI = 0.42–1.16, p = 0.16) and IgG (OR = 0.66, 95% CI = 0.42–105, p = 0.08) titers are not associative risk factors to lung cancer.
Immunoglobulin (IgA) and IgG seropositive titers of C. pneumoniae and lungs infected with HPV types 16 and 18 are potential risk factors associated with lung cancer.
Citation: Emmanuel Kwateng Drokow, Clement Yaw Effah, Clement Agboyibor, Jemima Twumwaah Budu, Francisca Arboh, Priscilla Akyaa Kyei-Baffour, Yao Xiao, Fan Zhang, Irene XY Wu. Microbial infections as potential risk factors for lung cancer: Investigating the role of human papillomavirus and chlamydia pneumoniae[J]. AIMS Public Health, 2023, 10(3): 627-646. doi: 10.3934/publichealth.2023044
Lung cancer is the leading cause of cancer morbidity and mortality worldwide. Apart from tobacco smoke and dietary factors, microbial infections have been reported as the third leading cause of cancers globally. Deciphering the association between microbiome and lung cancer will provide potential biomarkers and novel insight in lung cancer progression. In this current study, we performed a meta-analysis to decipher the possible association between C. pneumoniae and human papillomavirus (HPV) and the risk of lung cancer.
Literature search was conducted in most English and Chinese databases. Data were analyzed using CMA v.3.0 and RevMan v.5.3 software (Cochrane-Mantel-Haenszel method) by random-effects (DerSimonian and Laird) model.
The overall pooled estimates for HPV studies revealed that HPV infections in patients with lung cancer were significantly higher than those in the control group (OR = 2.33, 95% CI = 1.57–3.37, p < 0.001). Base on subgroup analysis, HPV infection rate was significantly higher in Asians (OR = 6.38, 95% CI = 2.33–17.46, p < 0.001), in tissues (OR = 5.04, 95% CI = 2.27–11.19, p < 0.001) and blood samples (OR = 1.40, 95% CI = 1.02–1.93, p = 0.04) of lung cancer patients but non-significantly lower in males (OR = 0.84, 95% CI = 0.57–1.22, p =0.35) and among lung cancer patients at clinical stage I-II (OR = 0.95, 95% CI = 0.61–1.49, p = 0.82). The overall pooled estimates from C. pneumoniae studies revealed that C. pneumoniae infection is a risk factor among lung cancer patients who are IgA seropositive (OR = 1.88, 95% CI = 1.30–2.70, p < 0.001) and IgG seropositive (OR = 1.50, 95% CI = 1.10–2.04, p = 0.010). All seronegative IgA (OR = 0.69, 95% CI = 0.42–1.16, p = 0.16) and IgG (OR = 0.66, 95% CI = 0.42–105, p = 0.08) titers are not associative risk factors to lung cancer.
Immunoglobulin (IgA) and IgG seropositive titers of C. pneumoniae and lungs infected with HPV types 16 and 18 are potential risk factors associated with lung cancer.

| [1] | Sung H, Ferlay J, Siegel RL, et al. (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71: 209-249. https://doi.org/10.3322/caac.21660 |
| [2] | Xiong WM, Xu QP, Li X, et al. (2017) The association between human papillomavirus infection and lung cancer: a system review and meta-analysis. Oncotarget 8: 96419. https://doi.org/10.18632/oncotarget.21682 |
| [3] | Denholm R, Schüz J, Straif K, et al. (2014) Is previous respiratory disease a risk factor for lung cancer?. Am J Respir Crit Care Med 190: 549-559. https://doi.org/10.1164/rccm.201402-0338OC |
| [4] | Zandberg DP, Bhargava R, Badin S, et al. (2013) The role of human papillomavirus in nongenital cancers. CA Cancer J Clin 63: 57-81. https://doi.org/10.3322/caac.21167 |
| [5] | (2007) IARC: Monographs on the evaluation of carcinogenic risks to humans. In: Human Papillomaviruses . Lyon: International Agency for Research on Cancer. https://doi.org/10.3322/caac.21167 |
| [6] | Tommasino M (2014) The human papillomavirus family and its role in carcinogenesis. Semin Cancer Biol 26: 13-21. https://doi.org/10.1016/j.semcancer.2013.11.002 |
| [7] | Srinivasan M, Taioli E, Ragin CC (2009) Human papillomavirus type 16 and 18 in primary lung cancers-a meta-analysis. Carcinogenesis 30: 1722-1728. https://doi.org/10.1093/carcin/bgp177 |
| [8] | Ragin C, Obikoya-Malomo M, Kim S, et al. (2014) HPV-associated lung cancers: an international pooled analysis. Carcinogenesis 35: 1267-1275. https://doi.org/10.1093/carcin/bgu038 |
| [9] | Jackson LA, Campbell LA, Schmidt RA, et al. (1997) Specificity of detection of Chlamydia pneumoniae in cardiovascular atheroma: evaluation of the innocent bystander hypothesis. Am J Pathol 150: 1785-1790. |
| [10] | Wong YK, Gallagher PJ, Ward ME (1999) Chlamydia pneumoniae and atherosclerosis. Heart 81: 232-238. https://doi.org/10.1136/hrt.81.3.232 |
| [11] | Jackson LA, Wang SP, Nazar-Stewart V, et al. (2000) Association of Chlamydia pneumoniae immunoglobulin A seropositivity and risk of lung cancer. Cancer Epidemiol Biomarkers Prev 9: 1263-1266. |
| [12] | Littman AJ, White E, Jackson LA, et al. (2004) Chlamydia pneumoniae infection and risk of lung cancer. Cancer Epidemiol Biomarkers Prev 13: 1624-1630. https://doi.org/10.1158/1055-9965.1624.13.10 |
| [13] | Kocazeybek B (2003) Chronic Chlamydophila pneumoniae infection in lung cancer, a risk factor: a case–control study. J Med Microbiol 52: 721-726. https://doi.org/10.1099/jmm.0.04845-0 |
| [14] | Smith JS, Kumlin U, Nyberg F, et al. (2008) Lack of association between serum antibodies of Chlamydia pneumoniae infection and the risk of lung cancer. Int J Cancer 123: 2469-2471. https://doi.org/10.1002/ijc.23814 |
| [15] | Koh WP, Chow VT, Phoon MC, et al. (2005) Lack of association between chronic Chlamydophila pneumoniae infection and lung cancer among nonsmoking Chinese women in Singapore. Int J Cancer 114: 502-504. https://doi.org/10.1002/ijc.20745 |
| [16] |
Moher D, Liberati A, Tetzlaff J, et al. (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (Chinese edition). Chin J Integr Med 7: 889-896. 
|
| [17] | Wells G A, Shea B, O'Connell D, et al. (2014) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Appl Eng Agric 18: 727-734. |
| [18] | Michael Borenstein, Larry V Hedges, Julian P T Higgins, et al. Introduction to Meta-Analysis-Part 4: heterogeneity (2009). Available form: https://onlinelibrary.wiley.com/doi/book/10.1002/9780470743386 |
| [19] | Luo GG, Ou JH (2015) Oncogenic viruses and cancer. Virol Sin 30: 83-84. https://doi.org/10.1007/s12250-015-3599-y |
| [20] | de Freitas AC, Gurgel AP, de Lima EG, et al. (2016) Human papillomavirus and lung cancinogenesis: an overview. J Cancer Res Clin Oncol 142: 2415-2427. https://doi.org/10.1007/s00432-016-2197-1 |
| [21] | Li G, He L, Zhang E, et al. (2011) Overexpression of human papillomavirus (HPV) type 16 oncoproteins promotes angiogenesis via enhancing HIF-1α and VEGF expression in non-small cell lung cancer cells. Cancer Lett 311: 160-170. https://doi.org/10.1016/j.canlet.2011.07.012 |
| [22] | Zhang E, Feng X, Liu F, et al. (2014) Roles of PI3K/Akt and c-Jun signaling pathways in human papillomavirus type 16 oncoprotein-induced HIF-1α, VEGF, and IL-8 expression and in vitro angiogenesis in non-small cell lung cancer cells. PloS one 9: e103440. https://doi.org/10.1371/journal.pone.0103440 |
| [23] | Liu F, Lin B, Liu X, et al. (2016) ERK signaling pathway is involved in HPV-16 E6 but not E7 oncoprotein-induced HIF-1α protein accumulation in NSCLC cells. Oncol Res 23: 109-118. https://doi.org/10.3727/096504015X14496932933610 |
| [24] | Willey JC, Broussoud A, Sleemi A, et al. (1991) Immortalization of normal human bronchial epithelial cells by human papillomaviruses 16 or 18. Cancer Res 51: 5370-5377. |
| [25] | Perrone F, Belluomini L, Mazzotta M, et al. (2021) Exploring the role of respiratory microbiome in lung cancer: a systematic review. Crit Rev Oncol Hematol 164: 103404. https://doi.org/10.1016/j.critrevonc.2021.103404 |
| [26] | Gori S, Inno A, Belluomini L, et al. (2019) Gut microbiota and cancer: How gut microbiota modulates activity, efficacy and toxicity of antitumoral therapy. Crit Rev Oncol Hematol 143: 139-147. https://doi.org/10.1016/j.critrevonc.2019.09.003 |
| [27] | Monroy-Iglesias MJ, Crescioli S, Beckmann K, et al. (2022) Antibodies as biomarkers for cancer risk: a systematic review. Clin Exp Immunol 209: 46-63. https://doi.org/10.1093/cei/uxac030 |
| [28] | Xiong WM, Xu QP, Li X, et al. (2017) The association between human papillomavirus infection and lung cancer: a system review and meta-analysis. Oncotarget 8: 96419-96432. https://doi.org/10.18632/oncotarget.21682 |
| [29] | Nadji SA, Mokhtari-Azad T, Mahmoodi M, et al. (2007) Relationship between lung cancer and human papillomavirus in north of Iran, Mazandaran province. Cancer Lett 248: 41-46. https://doi.org/10.1016/j.canlet.2006.05.016 |
| [30] | Yu Y, Yang A, Hu S, et al. (2013) Significance of human papillomavirus 16/18 infection in association with p53 mutation in lung carcinomas. Clin Respir J 7: 27-33. https://doi.org/10.1111/j.1752-699X.2011.00277.x |
| [31] |
Fei H E, Lin C A I (2014) Association of Chlamydia pneumoniae infection with risk of lung cancer. Chin J Public Health 30: 70-73.
|
| [32] | Klein F, Amin Kotb WF, Petersen I (2009) Incidence of human papilloma virus in lung cancer. Lung Cancer 65: 13-18. https://doi.org/10.1016/j.lungcan.2008.10.003 |
| [33] | Zhai K, Ding J, Shi HZ (2015) HPV and lung cancer risk: a meta-analysis. J Clin Virol 63: 84-90. https://doi.org/10.1016/j.jcv.2014.09.014 |
| [34] | Conceição Gomes Nascimento K, Gonçalves Lima É, Mota Nunes Z, et al. (2021) Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals. J Clin Med 10: 5209. https://doi.org/10.3390/jcm10215209 |
| [35] | Rezazadeh A, Laber DA, Ghim SJ, et al. (2009) The role of human papilloma virus in lung cancer: a review of the evidence. Am J Med Sci 338: 64-67. https://doi.org/10.1097/MAJ.0b013e3181a393ba |
| [36] | von Hertzen LC (1998) Chlamydia pneumoniae and its role in chronic obstructive pulmonary disease. Ann Med 30: 27-37. https://doi.org/10.3109/07853899808999382 |
| [37] | Burger MP, Hollema H, Gouw AS, et al. (1993) Cigarette smoking and human papillomavirus in patients with reported cervical cytological abnormality. BMJ 306: 749-752. https://doi.org/10.1136/bmj.306.6880.749 |
| [38] | Dubin S, Griffin D (2020) Lung cancer in non-smokers. Mo Med 117: 375-379. |
| [39] | Littman AJ, Jackson LA, Vaughan TL (2005) Chlamydia pneumoniae and lung cancer: epidemiologic evidence. Cancer Epidemiol Biomarkers Prev 14: 773-778. https://doi.org/10.1158/1055-9965.EPI-04-0599 |
| [40] | Geng Y., Shane R. B., Berencsi K., Gonczol E., Zaki M. H., Margolis D. J., Rook A. H. (2000) Chlamydia pneumoniae inhibits apoptosis in human peripheral blood mononuclear cells through induction of IL-10. J Immunol 164: 5522-5529. https://doi.org/10.4049/jimmunol.164.10.5522 |
| [41] | Laurila AL, Anttila T, Läärä E, et al. (1997) Serological evidence of an association between Chlamydia pneumoniae infection and lung cancer. Int J Cancer 74: 31-34. https://doi.org/10.1002/(sici)1097-0215(19970220)74:1<31::aid-ijc6>3.0.co;2-1 |
| [42] | Kol A, Sukhova GK, Lichtman AH, et al. (1998) Chlamydial heat shock protein 60 localizes in human atheroma and regulates macrophage tumor necrosis factor-α and matrix metalloproteinase expression. Circulation 98: 300-307. https://doi.org/10.1161/01.cir.98.4.300 |
| [43] | Moazed TC, Kuo C, Grayston JT (1997) Murine models of Chlamydia pneumoniae infection and atherosclerosis. J Infect Dis 175: 883-890. https://doi.org/10.1086/513986 |
| [44] | Redecke V, Dalhoff K, Bohnet S, et al. (1998) Interaction of Chlamydia pneumoniae and human alveolar macrophages: infection and inflammatory response. Am J Respir Cell Mol Biol 19: 721-727. https://doi.org/10.1165/ajrcmb.19.5.3072 |
| [45] | Smith JS, Kumlin U, Nyberg F, et al. (2008) Lack of association between serum antibodies of Chlamydia pneumoniae infection and the risk of lung cancer. Int J Cancer 123: 2469-2471. https://doi.org/10.1002/ijc.23814 |
| [46] | Zhan P, Suo LJ, Qian Q, et al. (2011) Chlamydia pneumoniae infection and lung cancer risk: a meta-analysis. Eur J Cancer 47: 742-747. https://doi.org/10.1016/j.ejca.2010.11.003 |
| [47] | Zakhour MD J, Muller D, Glynn A, et al. (2021) Association of Lung cancer with Pneumonia and Chlamydia pneumoniae infection. Univ Louisville J Respir Infect 6: 8. https://doi.org/10.55504/2473-2869.1227 |
| [48] | Wang C, Zhang N, Gao L (2019) Association between Chlamydia pneumoniae infection and lung cancer: a meta-analysis. Transl Cancer Res 8: 2813-2019. https://doi.org/10.21037/tcr.2019.10.35 |
| [49] | Xu X, Liu Z, Xiong W, et al. (2020) Combined and interaction effect of chlamydia pneumoniae infection and smoking on lung cancer: a case-control study in Southeast China. BMC cancer 20: 903. https://doi.org/10.1186/s12885-020-07418-8 |
| [50] | Kalay N, Kutukoglu I, Ozdogru I, et al. (2008) The relationship between Chlamydophila pneumoniae IgG titer and coronary atherosclerosis. Cardiol J 15: 245-251. |
| [51] | Lu Q, Xu J, Liu H (2009) Association between Chlamydia pneumoniae IgG antibodies and migraine. J Headache Pain 10: 121-124. https://doi.org/10.1007/s10194-009-0096-4 |
| [52] | Karvonen M, Tuomilehto J, Pitkäniemi J, et al. (1994) Importance of smoking for Chlamydia pneumoniae seropositivity. Int J Epidemiol 23: 1315-1321. https://doi.org/10.1093/ije/23.6.1315 |
| [53] | Hahn DL, Golubjatnikov R (1992) Smoking is a potential confounder of the Chlamydia pneumoniae-coronary artery disease association. Arterioscler Thromb 12: 945-947. https://doi.org/10.1161/01.atv.12.8.945 |
| [54] | McDermott A (2023) Microbiome insights open new avenues to treat HPV. Proc Natl Acad Sci USA 120: e2304645120. https://doi.org/10.1073/pnas.2304645120 |
| [55] | Oyouni AAA (2023) Human papillomavirus in cancer: Infection, disease transmission, and progress in vaccines. J Infect Public Health 16: 626-631. https://doi.org/10.1016/j.jiph.2023.02.014 |
| [56] | Coccia M (2014) Path-breaking target therapies for lung cancer and a far-sighted health policy to support clinical and cost effectiveness. Health Policy Techn 3: 74-82. https://doi.org/10.1016/j.hlpt.2013.09.007 |
| [57] | Carlander C, Brännström J, Månsson F, et al. (2023) Cohort profile: InfCareHIV, a prospective registry-based cohort study of people with diagnosed HIV in Sweden. BMJ Open 13: e069688. https://doi.org/10.1136/bmjopen-2022-069688 |
| [58] | Rojas L, Mayorga D, Ruiz-Patiño A, et al. (2022) Human papillomavirus infection and lung adenocarcinoma: special benefit is observed in patients treated with immune checkpoint inhibitors. ESMO Open 7: 100500. https://doi.org/10.1016/j.esmoop.2022.100500 |
| [59] | Wang JL, Lee WJ, Fang CL, et al. (2022) Human Papillomavirus Oncoproteins Confer Sensitivity to Cisplatin by Interfering with Epidermal Growth Factor Receptor Nuclear Trafficking Related to More Favorable Clinical Survival Outcomes in Non-Small Cell Lung Cancer. Cancers (Basel) 14: 5333. https://doi.org/10.3390/cancers14215333 |
| [60] | Huang JY, Lin C, Tsai SC, et al. (2022) Human Papillomavirus Is Associated With Adenocarcinoma of Lung: A Population-Based Cohort Study. Front Med (Lausanne) 30: 932196. https://doi.org/10.3389/fmed.2022.932196 |
| [61] | Budisan L, Zanoaga O, Braicu C, et al. (2021) Links between Infections, Lung Cancer, and the Immune System. Int J Mol Sci 22: 9394. https://doi.org/10.3390/ijms22179394 |
| [62] | Cho WC, Kwan CK, Yau S, et al. (2011) The role of inflammation in the pathogenesis of lung cancer. Expert Opin Ther Targets 15: 1127-1137. https://doi.org/10.1517/14728222.2011.599801 |
| [63] | Tan Z, Xue H, Sun Y, et al. (2021) The role of tumor inflammatory microenvironment in lung cancer. Front Pharmacol 12: 688625. https://doi.org/10.3389/fphar.2021.688625 |
| [64] | Khusnurrokhman G, Wati FF (2022) Tumor-promoting inflammation in lung cancer: a literature review. Ann Med Surg (Lond) 79: 104022. https://doi.org/10.1016/j.amsu.2022.104022 |
| [65] | Hu Y, Ren S, He Y, et al. (2020) Possible oncogenic viruses associated with lung cancer. Onco Targets Ther 13: 10651-10666. https://doi.org/10.2147/OTT.S263976 |
| [66] | Prasad SK, Bhat S, Shashank D, et al. (2022) Bacteria-mediated oncogenesis and the underlying molecular intricacies: What we know so far. Front Oncol 12: 836004. https://doi.org/10.3389/fonc.2022.836004 |
| [67] | Premachandra NM, Jayaweera JAAS (2022) Chlamydia pneumoniae infections and development of lung cancer: systematic review. Infect Agent Cancer 17: 11. https://doi.org/10.1186/s13027-022-00425-3 |
| [68] | Yusuf K, Sampath V, Umar S (2023) Bacterial Infections and Cancer: Exploring This Association And Its Implications for Cancer Patients. Int J Mol Sci 24: 3110. https://doi.org/10.3390/ijms24043110 |
| [69] | El Bagoury M, Fahmy M (2022) The Epidemiology of Lung Cancer-How Much Have We Discovered?. J Pharm Res Int 34: 23-33. https://doi.org/10.9734/jpri/2022/v34i48A36414 |
 publichealth-10-03-044-s001.pdf publichealth-10-03-044-s001.pdf |
 |




Figures(5) / Tables(3)

Emmanuel Kwateng Drokow, Clement Yaw Effah, Clement Agboyibor, Jemima Twumwaah Budu, Francisca Arboh, Priscilla Akyaa Kyei-Baffour, Yao Xiao, Fan Zhang, Irene XY Wu. Microbial infections as potential risk factors for lung cancer: Investigating the role of human papillomavirus and chlamydia pneumoniae[J]. AIMS Public Health, 2023, 10(3): 627-646. doi: 10.3934/publichealth.2023044







 DownLoad:
DownLoad: