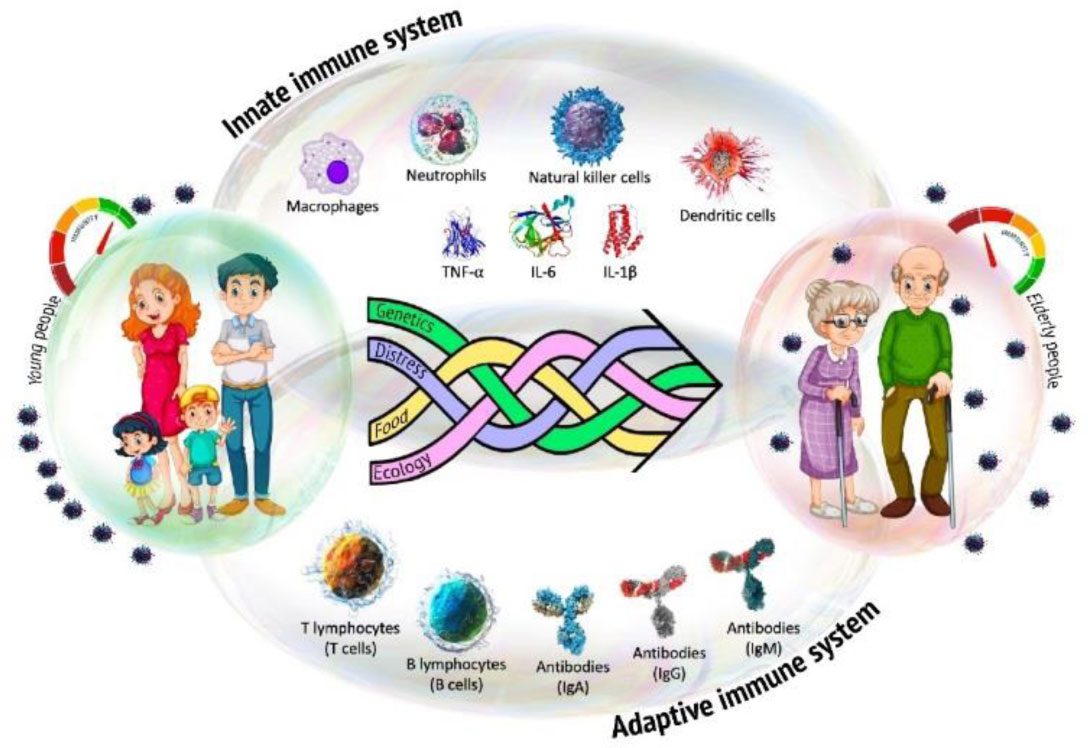
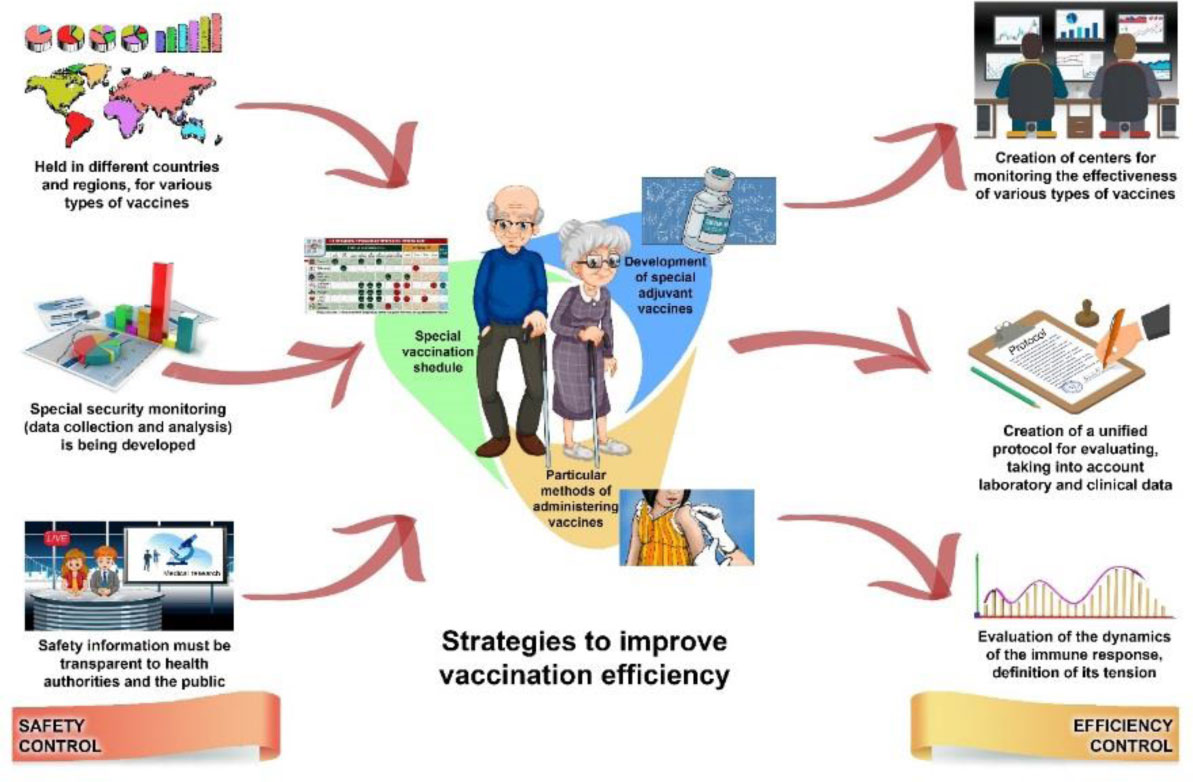
In December 2020, COVID-19 vaccination started in many countries, with which the world community hopes to stop the further spread of the current pandemic. More than 90% of sick and deceased patients belong to the category of older adults (65 years and older). This category of the population is most vulnerable to infectious diseases, so vaccination is the most effective preventive strategy, the need for which for older adults is indisputable. Here we briefly summarize information about age-related changes in the immune system and present current data on their impact on the formation of the immune response to vaccination. Older age is accompanied by the process of biological aging accompanied by involution of the immune system with increased susceptibility to infections and a decrease in the effect of immunization. Therefore, in the ongoing mass COVID-19 vaccination, the older adults are a growing public health concern. The authors provide an overview of the various types of COVID-19 vaccines approved for mass immunization of the population by the end of 2020, including older adults, as well as an overview of strategies and platforms to improve the effectiveness of vaccination of this population. In the final part, the authors propose for discussion a system for assessing the safety and monitoring the effectiveness of COVID-19 vaccines for the older adults.
Citation: Boris G Andryukov, Natalya N Besednova. Older adults: panoramic view on the COVID-19 vaccination[J]. AIMS Public Health, 2021, 8(3): 388-415. doi: 10.3934/publichealth.2021030
In December 2020, COVID-19 vaccination started in many countries, with which the world community hopes to stop the further spread of the current pandemic. More than 90% of sick and deceased patients belong to the category of older adults (65 years and older). This category of the population is most vulnerable to infectious diseases, so vaccination is the most effective preventive strategy, the need for which for older adults is indisputable. Here we briefly summarize information about age-related changes in the immune system and present current data on their impact on the formation of the immune response to vaccination. Older age is accompanied by the process of biological aging accompanied by involution of the immune system with increased susceptibility to infections and a decrease in the effect of immunization. Therefore, in the ongoing mass COVID-19 vaccination, the older adults are a growing public health concern. The authors provide an overview of the various types of COVID-19 vaccines approved for mass immunization of the population by the end of 2020, including older adults, as well as an overview of strategies and platforms to improve the effectiveness of vaccination of this population. In the final part, the authors propose for discussion a system for assessing the safety and monitoring the effectiveness of COVID-19 vaccines for the older adults.

| [1] | United Nations: Department of Economic and Social Affairs, Population Division (2019) World Population Prospects 2019: Highlights (ST/ESA/SER.A/423) United Nations New York: Available from: https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf. |
| [2] | United Nations: Department of Economic and Social Affairs Population Dynamics World Population Prospects 2019 Available from: https://population.un.org/wpp/DataQuery/. |
| [3] |
Bektas A, Schurman SH, Sen R, et al. (2017) Human T cell immunosenescence and inflammation in aging. J Leukoc Biol 102: 977-988. doi: 10.1189/jlb.3RI0716-335R

|
| [4] |
Austad SN, Hoffman JM (2018) Is antagonistic pleiotropy ubiquitous in aging biology? Evol Med Public Hlth 2018: 287-294. doi: 10.1093/emph/eoy033
|
| [5] |
Fülöp T, Larbi A, Witkowski JM (2019) Human Inflammaging. Gerontology 65: 495-504. doi: 10.1159/000497375
|
| [6] |
Pinti M, Appay V, Campisi J, et al. (2016) Aging of the immune system: Focus on inflammation and vaccination. Eur J Immunol 46: 2286-2301. doi: 10.1002/eji.201546178
|
| [7] |
Oh SJ, Lee JK, Shin OS (2019) Aging and the Immune System: The Impact of Immunosenescence on Viral Infection, Immunity and Vaccine Immunogenicity. Immune Netw 19: e37. doi: 10.4110/in.2019.19.e37
|
| [8] |
Crooke SN, Ovsyannikova IG, Poland GA, et al. (2019) Immunosenescence and human vaccine immune responses. Immun Ageing 16: 25. doi: 10.1186/s12979-019-0164-9
|
| [9] | World Health Organization COVID-19 vaccines Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines. |
| [10] | Center for Disease Control and Prevention Weekly Updates by Select Demographic and Geographic Characteristics Available from: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#AgeAndSex. |
| [11] |
Molinari NA, Ortega-Sanchez IR, Messonnier ML, et al. (2007) The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine 25: 5086-5096. doi: 10.1016/j.vaccine.2007.03.046
|
| [12] |
Gralinski LE, Menachery VD (2020) Return of the Coronavirus: 2019-nCoV. Viruses 12: 135. doi: 10.3390/v12020135
|
| [13] |
Cianci R, Franza L, Massaro MG, et al. (2020) The Interplay between Immunosenescence and Microbiota in the Efficacy of Vaccines. Vaccines (Basel) 8: 636. doi: 10.3390/vaccines8040636
|
| [14] | Zhang Y, Zeng G, Pan H, et al. (2020) Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18-59 years: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect Dis S1473–3099: 30987. |
| [15] |
Xia S, Zhang Y, Wang Y, et al. (2020) Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect Dis 21: 39-51. doi: 10.1016/S1473-3099(20)30831-8
|
| [16] |
Thompson HL, Smithey MJ, Surh CD, et al. (2020) Functional and Homeostatic Impact of Age-Related Changes in Lymph Node Stroma. Front Immunol 8: 706. doi: 10.3389/fimmu.2017.00706
|
| [17] |
Song CY, Xu J, He JQ, et al. (2020) Immune dysfunction following COVID-19, especially in severe patients. Sci Rep 10: 15838. doi: 10.1038/s41598-020-72718-9
|
| [18] |
Connors J, Bell MR, Marcy J, et al. (2021) The impact of immuno-aging on SARS-CoV-2 vaccine development. Geroscience 43: 31-51. doi: 10.1007/s11357-021-00323-3
|
| [19] |
Arvey A, Rowe M, Legutki JB, et al. (2020) Age-associated changes in the circulating human antibody repertoire are upregulated in autoimmunity. Immun Ageing 17: 28. doi: 10.1186/s12979-020-00193-x
|
| [20] |
Frawley T, van Gelderen F, Somanadhan S, et al. (2020) The impact of COVID-19 on health systems, mental health and the potential for nursing. Ir J Psychol Med 16: 1-7. doi: 10.1017/ipm.2020.105
|
| [21] |
Ponnappan S, Ponnappan U (2011) Aging and immune function: molecular mechanisms to interventions. Antioxid Redox Signal 14: 1551-1585. doi: 10.1089/ars.2010.3228
|
| [22] |
Solana R, Pawelec G, Tarazona R (2006) Aging and innate immunity. Immunity 24: 491-494. doi: 10.1016/j.immuni.2006.05.003
|
| [23] |
Ferrucci L, Fabbri E (2018) Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol 15: 505-522. doi: 10.1038/s41569-018-0064-2
|
| [24] |
Gubbels Bupp MR, Potluri T, Fink AL, et al. (2018) The Confluence of Sex Hormones and Aging on Immunity. Front Immunol 9: 1269. doi: 10.3389/fimmu.2018.01269
|
| [25] |
van Eeden C, Khan L, Osman MS, et al. (2020) Natural Killer Cell Dysfunction and Its Role in COVID-19. Int J Mol Sci 21: 6351. doi: 10.3390/ijms21176351
|
| [26] |
Przemska-Kosicka A, Childs CE, Maidens C, et al. (2018) Age-Related Changes in the Natural Killer Cell Response to Seasonal Influenza Vaccination Are Not Influenced by a Synbiotic: a Randomised Controlled Trial. Front Immunol 9: 591. doi: 10.3389/fimmu.2018.00591
|
| [27] |
Guo H, Kumar P, Moran TM, et al. (2009) The functional impairment of natural killer cells during influenza virus infection. Immunol Cell Biol 87: 579-589. doi: 10.1038/icb.2009.60
|
| [28] |
Fulop T, Witkowski JM, Le Page A, et al. (2017) Intracellular signalling pathways: targets to reverse immunosenescence. Clin Exp Immunol 187: 35-43. doi: 10.1111/cei.12836
|
| [29] |
Zhou R, To KK, Wong YC, et al. (2020) Acute SARS-CoV-2 Infection Impairs Dendritic Cell and T Cell Responses. Immunity 53: 864-877. doi: 10.1016/j.immuni.2020.07.026
|
| [30] |
Fulop T, Larbi A, Dupuis G, et al. (2018) Immunosenescence and Inflamm-Aging as Two Sides of the Same Coin: Friends or Foes? Front Immunol 8: 1960. doi: 10.3389/fimmu.2017.01960
|
| [31] |
Iberg CA, Jones A, Hawiger D (2017) Dendritic Cells As Inducers of Peripheral Tolerance. Trends Immunol 38: 793-804. doi: 10.1016/j.it.2017.07.007
|
| [32] |
Ray D, Yung R (2018) Immune senescence, epigenetics and autoimmunity. Clin Immunol 196: 59-63. doi: 10.1016/j.clim.2018.04.002
|
| [33] |
Agrawal A, Sridharan A, Prakash S, et al. (2012) Dendritic cells and aging: consequences for autoimmunity. Expert Rev Clin Immunol 8: 73-80. doi: 10.1586/eci.11.77
|
| [34] |
Agrawal A, Agrawal S, Gupta S (2017) Role of Dendritic Cells in Inflammation and Loss of Tolerance in the Elderly. Front Immunol 8: 896. doi: 10.3389/fimmu.2017.00896
|
| [35] | Agrawal A, Agrawal S, Gupta S (2018) Role of Dendritic Cells in Aging. Handbook of Immunosenescence Cham: Springer. |
| [36] |
Blanco-Melo D, Nilsson-Payant BE, Liu WC, et al. (2020) Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 181: 1036-1045. doi: 10.1016/j.cell.2020.04.026
|
| [37] |
Schröder AK, Rink L (2003) Neutrophil immunity of the elderly. Mech Ageing Dev 124: 419-425. doi: 10.1016/S0047-6374(03)00017-4
|
| [38] |
Butcher S, Chahel H, Lord JM (2000) Review article: ageing and the neutrophil: no appetite for killing? Immunology 100: 411-416. doi: 10.1046/j.1365-2567.2000.00079.x
|
| [39] |
Naccache PH, Lefebvre JS (2014) A straight neutrophil path to healthy aging? Blood 123: 154-156. doi: 10.1182/blood-2013-11-538256
|
| [40] |
Mócsai A (2013) Diverse novel functions of neutrophils in immunity, inflammation, and beyond. J Exp Med 210: 1283-1299. doi: 10.1084/jem.20122220
|
| [41] |
Dinauer MC (2014) Disorders of neutrophil function: an overview. Methods Mol Biol 1124: 501-515. doi: 10.1007/978-1-62703-845-4_30
|
| [42] |
Ferrucci L, Fabbri E (2018) Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol 15: 505-522. doi: 10.1038/s41569-018-0064-2
|
| [43] |
Aiello A, Farzaneh F, Candore G, et al. (2019) Immunosenescence and Its Hallmarks: How to Oppose Aging Strategically? A Review of Potential Options for Therapeutic Intervention. Front Immunol 10: 2247. doi: 10.3389/fimmu.2019.02247
|
| [44] |
Rubtsov AV, Rubtsova K, Fischer A, et al. (2011) Toll-like receptor 7 (TLR7)-driven accumulation of a novel CD11c(+) B-cell population is important for the development of autoimmunity. Blood 118: 1305-1315. doi: 10.1182/blood-2011-01-331462
|
| [45] |
Bektas A, Schurman SH, Sen R, et al. (2017) Human T cell immunosenescence and inflammation in aging. J Leukoc Biol 102: 977-988. doi: 10.1189/jlb.3RI0716-335R
|
| [46] | Tu W, Rao S (2016) Mechanisms Underlying T Cell Immunosenescence: Aging and Cytomegalovirus Infection. Front Microbiol 7: 2111. |
| [47] |
Gustafson CE, Kim C, Weyand CM, et al. (2020) Influence of immune aging on vaccine responses. J Allergy Clin Immunol 145: 1309-1321. doi: 10.1016/j.jaci.2020.03.017
|
| [48] |
Park S, Nahm MH (2011) Older adults have a low capacity to opsonize pneumococci due to low IgM antibody response to pneumococcal vaccinations. Infect Immun 79: 314-320. doi: 10.1128/IAI.00768-10
|
| [49] |
Zhu FC, Guan XH, Li YH, et al. (2020) Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 396: 479-488. doi: 10.1016/S0140-6736(20)31605-6
|
| [50] | Schenkelberg T (2020) Vaccine-induced protection in aging adults and pandemic response. Biochem Biophys Res Commun S0006-291X(20)32020-9. |
| [51] |
Ruan Q, Yang K, Wang W, et al. (2020) Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med 46: 846-848. doi: 10.1007/s00134-020-05991-x
|
| [52] |
McElhaney JE, Coler RN, Baldwin SL (2013) Immunologic correlates of protection and potential role for adjuvants to improve influenza vaccines in older adults. Expert Rev Vaccines 12: 759-766. doi: 10.1586/14760584.2013.811193
|
| [53] |
Huff WX, Kwon JH, Henriquez M, et al. (2019) The Evolving Role of CD8+CD28- Immunosenescent T Cells in Cancer Immunology. Int J Mol Sci 20: 2810. doi: 10.3390/ijms20112810
|
| [54] |
McElhaney JE, Verschoor CP, Andrew MK, et al. (2020) The immune response to influenza in older humans: beyond immune senescence. Immun Ageing 17: 10. doi: 10.1186/s12979-020-00181-1
|
| [55] |
Saletti G, Gerlach T, Jansen JM, et al. (2020) Older adults lack SARS CoV-2 cross-reactive T-lymphocytes directed to human coronaviruses OC43 and NL63. Sci Rep 10: 21447. doi: 10.1038/s41598-020-78506-9
|
| [56] |
Ma S, Wang C, Mao X, et al. (2019) B Cell Dysfunction Associated with Aging and Autoimmune Diseases. Front Immunol 10: 318. doi: 10.3389/fimmu.2019.00318
|
| [57] |
Cancro MP, Hao Y, Scholz JL, et al. (2009) B cells and aging: molecules and mechanisms. Trends Immunol 30: 313-318. doi: 10.1016/j.it.2009.04.005
|
| [58] |
Phalke S, Marrack P (2018) Age (autoimmunity) associated B cells (ABCs) and their relatives. Curr Opin Immunol 55: 75-80. doi: 10.1016/j.coi.2018.09.007
|
| [59] |
Bulati M, Caruso C, Colonna-Romano G (2017) From lymphopoiesis to plasma cells differentiation, the age-related modifications of B cell compartment are influenced by “inflamm-ageing”. Ageing Res Rev 36: 125-136. doi: 10.1016/j.arr.2017.04.001
|
| [60] |
Du SW, Arkatkar T, Jacobs HM, et al. (2019) Generation of functional murine CD11c+ age-associated B cells in the absence of B cell T-bet expression. Eur J Immunol 49: 170-178. doi: 10.1002/eji.201847641
|
| [61] |
Du SW, Arkatkar T, Al Qureshah F, et al. (2019) Functional Characterization of CD11c+ Age-Associated B Cells as Memory B Cells. J Immunol 203: 2817-2826. doi: 10.4049/jimmunol.1900404
|
| [62] |
Karnell JL, Kumar V, Wang J, et al. (2017) Role of CD11c+ T-bet+ B cells in human health and disease. Cell Immunol 321: 40-45. doi: 10.1016/j.cellimm.2017.05.008
|
| [63] |
Sachinidis A, Xanthopoulos K, Garyfallos A (2020) Age-Associated B Cells (ABCs) in the Prognosis, Diagnosis and Therapy of Systemic Lupus Erythematosus (SLE). Mediterr J Rheumatol 31: 311-318. doi: 10.31138/mjr.31.3.311
|
| [64] |
Hartley GE, Edwards ESJ, Aui PM, et al. (2020) Rapid generation of durable B cell memory to SARS-CoV-2 spike and nucleocapsid proteins in COVID-19 and convalescence. Sci Immunol 5: eabf8891. doi: 10.1126/sciimmunol.abf8891
|
| [65] |
Cañete PF, Vinuesa CG (2020) COVID-19 Makes B Cells Forget, but T Cells Remember. Cell 183: 13-15. doi: 10.1016/j.cell.2020.09.013
|
| [66] |
Sosa-Hernández VA, Torres-Ruíz J, Cervantes-Díaz R, et al. (2020) B Cell Subsets as Severity-Associated Signatures in COVID-19 Patients. Front Immunol 11: 611004. doi: 10.3389/fimmu.2020.611004
|
| [67] |
Hao Y, O'Neill P, Naradikian MS, et al. (2011) A B-cell subset uniquely responsive to innate stimuli accumulates in aged mice. Blood 118: 1294-304. doi: 10.1182/blood-2011-01-330530
|
| [68] |
Park S, Nahm MH (2011) Older adults have a low capacity to opsonize pneumococci due to low IgM antibody response to pneumococcal vaccinations. Infect Immun 79: 314-320. doi: 10.1128/IAI.00768-10
|
| [69] |
Smetana J, Chlibek R, Shaw J, et al. (2018) Influenza vaccination in the elderly. Hum Vaccin Immunother 14: 540-549. doi: 10.1080/21645515.2017.1343226
|
| [70] |
Kwong JC, Campitelli MA, Gubbay JB, et al. (2013) Vaccine effectiveness against laboratory-confirmed influenza hospitalizations among elderly adults during the 2010-2011 season. Clin Infect Dis 57: 820-827. doi: 10.1093/cid/cit404
|
| [71] |
Bonmarin I, Belchior E, Lévy-Bruhl D (2015) Impact of influenza vaccination on mortality in the French elderly population during the 2000–2009 period. Vaccine 33: 1099-1101. doi: 10.1016/j.vaccine.2015.01.023
|
| [72] |
Chiu C (2016) Seasonal influenza vaccines and hurdles to mutual protection. Clin Microbiol Infect 22: S113-S119. doi: 10.1016/j.cmi.2016.03.021
|
| [73] | Koldaş ZL (2017) Yaşlı popülasyonda bağışıklama (aşılama) [Vaccination in the elderly population]. Turk Kardiyol Dern Ars 45: 124-127. |
| [74] |
Derhovanessian E, Pawelec G (2012) Vaccination in the elderly. Microb Biotechnol 5: 226-232. doi: 10.1111/j.1751-7915.2011.00283.x
|
| [75] | World Health Organization The COVID-19 candidate vaccine landscape and tracker Available from: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines. |
| [76] | World Health Organization COVID-19 vaccines Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines?. |
| [77] | Precision vaccinations EpiVacCorona Vaccine Available from: https://www.precisionvaccinations.com/vaccines/epivaccorona-vaccine. |
| [78] | Novavax Coronavirus Vaccine Candidate Updates Available from: https://www.novavax.com/covid-19-coronavirus-vaccine-candidate-updates. |
| [79] |
Keech C, Albert G, Cho I, et al. (2020) Phase 1-2 Trial of a SARS-CoV-2 Recombinant Spike Protein Nanoparticle Vaccine. N Engl J Med 383: 2320-2332. doi: 10.1056/NEJMoa2026920
|
| [80] | Dai L, Gao GF (2020) Viral targets for vaccines against COVID-19. Nat Rev Immunol 18: 1-10. |
| [81] |
Balakrishnan VS (2020) The arrival of Sputnik V. Lancet Infect Dis 20: 1128. doi: 10.1016/S1473-3099(20)30709-X
|
| [82] | Sputnik V GENERAL INFORMATION Available from: https://sputnikvaccine.com/rus/about-vaccine/. |
| [83] | Johnson & Johnson Johnson & Johnson Initiates Pivotal Global Phase 3 Clinical Trial of Janssen's COVID-19 Vaccine Candidate Available from: https://www.jnj.com/johnson-johnson-initiates-pivotal-global-phase-3-clinical-trial-of-janssens-covid-19-vaccine-candidate. |
| [84] | Knoll MD, Wonodi C (2020) Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet S0140-6736(20)32623-4. |
| [85] |
Tanne JH (2020) Covid-19: Pfizer-BioNTech vaccine is rolled out in US. BMJ 371: m4836. doi: 10.1136/bmj.m4836
|
| [86] | Centers for Disease Control and Prevention (CDC) Moderna COVID-19 Vaccine Available from: https://www.cdc.gov/vaccines/covid-19/info-by-product/moderna/index.html. |
| [87] | BioRender COVID-19 Vaccine & Therapeutics Tracker Available from: https://biorender.com/covid-vaccine-tracker. |
| [88] |
Coelingh K, Olajide IR, MacDonald P, et al. (2015) Efficacy and effectiveness of live attenuated influenza vaccine in school-age children. Expert Rev Vaccines 14: 1331-1346. doi: 10.1586/14760584.2015.1078732
|
| [89] |
Singanayagam A, Zambon M, Lalvani A, et al. (2018) Urgent challenges in implementing live attenuated influenza vaccine. Lancet Infect Dis 18: e25-e32. doi: 10.1016/S1473-3099(17)30360-2
|
| [90] |
Chua BY, Sekiya T, Jackson DC (2018) Opinion: Making Inactivated and Subunit-Based Vaccines Work. Viral Immunol 31: 150-158. doi: 10.1089/vim.2017.0146
|
| [91] |
Brickley EB, Wright PF (2017) Maximising the impact of inactivated polio vaccines. Lancet Infect Dis 17: 680-681. doi: 10.1016/S1473-3099(17)30236-0
|
| [92] |
Tripathi NK, Shrivastava A (2018) Recent Developments in Recombinant Protein-Based Dengue Vaccines. Front Immunol 9: 1919. doi: 10.3389/fimmu.2018.01919
|
| [93] |
de Vries RD, Rimmelzwaan GF (2016) Viral vector-based influenza vaccines. Hum Vaccin Immunother 12: 2881-2901. doi: 10.1080/21645515.2016.1210729
|
| [94] |
Logunov DY, Dolzhikova IV, Zubkova OV, et al. (2020) Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia. Lancet 396: 887-897. doi: 10.1016/S0140-6736(20)31866-3
|
| [95] |
Humphreys IR, Sebastian S (2018) Novel viral vectors in infectious diseases. Immunology 153: 1-9. doi: 10.1111/imm.12829
|
| [96] |
Dalmo RA (2018) DNA vaccines for fish: Review and perspectives on correlates of protection. J Fish Dis 41: 1-9. doi: 10.1111/jfd.12727
|
| [97] |
Tanne JH (2020) Covid-19: Pfizer-BioNTech vaccine is rolled out in US. BMJ 371: m4836. doi: 10.1136/bmj.m4836
|
| [98] |
Lundstrom K (2020) Self-Amplifying RNA Viruses as RNA Vaccines. Int J Mol Sci 21: 5130. doi: 10.3390/ijms21145130
|
| [99] |
Dong Y, Dai T, Wei Y, et al. (2020) A systematic review of SARS-CoV-2 vaccine candidates. Signal Transduct Target Ther 5: 237. doi: 10.1038/s41392-020-00352-y
|
| [100] |
Armengaud J, Delaunay-Moisan A, Thuret JY, et al. (2020) The importance of naturally attenuated SARS-CoV-2 in the fight against COVID-19. Environ Microbiol 22: 1997-2000. doi: 10.1111/1462-2920.15039
|
| [101] |
Alsulaiman JW, Khasawneh AI, Kheirallah KA (2020) Could “trained immunity” be induced by live attenuated vaccines protect against COVID-19? Review of available evidence. J Infect Dev Ctries 14: 957-962. doi: 10.3855/jidc.12805
|
| [102] | Fidel PL, Noverr MC (2020) Could an Unrelated Live Attenuated Vaccine Serve as a Preventive Measure To Dampen Septic Inflammation Associated with COVID-19 Infection? mBio 11: e00907-e00920. |
| [103] |
Roukens AH, Soonawala D, Joosten SA, et al. (2011) Elderly subjects have a delayed antibody response and prolonged viraemia following yellow fever vaccination: a prospective controlled cohort study. PLoS One 6: e27753. doi: 10.1371/journal.pone.0027753
|
| [104] |
Monath TP, Cetron MS, McCarthy K, et al. (2005) Yellow fever 17D vaccine safety and immunogenicity in the elderly. Hum Vaccin 1: 207-214. doi: 10.4161/hv.1.5.2221
|
| [105] |
Al-Kassmy J, Pedersen J, Kobinger G (2020) Vaccine Candidates against Coronavirus Infections. Where Does COVID-19 Stand? Viruses 12: 861. doi: 10.3390/v12080861
|
| [106] |
Locht C (2020) Vaccines against COVID-19. Anaesth Crit Care Pain Med 39: 703-705. doi: 10.1016/j.accpm.2020.10.006
|
| [107] |
Wagner A, Garner-Spitzer E, Jasinska J, et al. (2018) Age-related differences in humoral and cellular immune responses after primary immunisation: indications for stratified vaccination schedules. Sci Rep 8: 9825. doi: 10.1038/s41598-018-28111-8
|
| [108] |
Dugan HL, Henry C, Wilson PC (2020) Aging and influenza vaccine-induced immunity. Cell Immunol 348: 103998. doi: 10.1016/j.cellimm.2019.103998
|
| [109] |
van den Berg SPH, Wong A, Hendriks M, et al. (2018) Negative Effect of Age, but Not of Latent Cytomegalovirus Infection on the Antibody Response to a Novel Influenza Vaccine Strain in Healthy Adults. Front Immunol 9: 82. doi: 10.3389/fimmu.2018.00082
|
| [110] |
Farina SF, Gao GP, Xiang ZQ, et al. (2001) Replication-defective vector based on a chimpanzee adenovirus. J Virol 75: 11603-11613. doi: 10.1128/JVI.75.23.11603-11613.2001
|
| [111] |
Tatsis N, Ertl HC (2004) Adenoviruses as vaccine vectors. Mol Ther 10: 616-629. doi: 10.1016/j.ymthe.2004.07.013
|
| [112] |
Vogels R, Zuijdgeest D, van Rijnsoever R, et al. (2003) Replication-deficient human adenovirus type 35 vectors for gene transfer and vaccination: efficient human cell infection and bypass of preexisting adenovirus immunity. J Virol 77: 8263-8271. doi: 10.1128/JVI.77.15.8263-8271.2003
|
| [113] |
Nidetz NF, McGee MC, Tse LV, et al. (2020) Adeno-associated viral vector-mediated immune responses: Understanding barriers to gene delivery. Pharmacol Ther 207: 107453. doi: 10.1016/j.pharmthera.2019.107453
|
| [114] |
Hinz T, Kallen K, Britten CM, et al. (2017) The European Regulatory Environment of RNA-Based Vaccines. Methods Mol Biol 1499: 203-222. doi: 10.1007/978-1-4939-6481-9_13
|
| [115] |
Plotkin S (2014) History of vaccination. Proc Natl Acad Sci USA 111: 12283-12287. doi: 10.1073/pnas.1400472111
|
| [116] |
Dalmo RA (2018) DNA vaccines for fish: Review and perspectives on correlates of protection. J Fish Dis 41: 1-9. doi: 10.1111/jfd.12727
|
| [117] |
Tanne JH (2020) Covid-19: Pfizer-BioNTech vaccine is rolled out in US. BMJ 371: m4836. doi: 10.1136/bmj.m4836
|
| [118] |
Lundstrom K (2020) Self-Amplifying RNA Viruses as RNA Vaccines. Int J Mol 21: 5130. doi: 10.3390/ijms21145130
|
| [119] |
Broderick KE, Humeau LM (2017) Enhanced Delivery of DNA or RNA Vaccines by Electroporation. Methods Mol Biol 1499: 193-200. doi: 10.1007/978-1-4939-6481-9_12
|
| [120] |
Zheng Z, Diaz-Arévalo D, Guan H, et al. (2018) Noninvasive vaccination against infectious diseases. Hum Vaccin Immunother 14: 1717-1733. doi: 10.1080/21645515.2018.1461296
|
| [121] | Moderna Moderna's Company History Available from: https://www.modernatx.com/about-us/moderna-facts. |
| [122] |
Soiza RL, Scicluna C, Thomson EC (2021) Efficacy and safety of COVID-19 vaccines in older people. Age Ageing 50: 279-283. doi: 10.1093/ageing/afaa274
|
| [123] |
Di Pasquale A, Preiss S, Tavares Da Silva F, et al. (2015) Vaccine Adjuvants: from 1920 to 2015 and Beyond. Vaccines (Basel) 3: 320-343. doi: 10.3390/vaccines3020320
|
| [124] |
Zepp F (2010) Principles of vaccine design-Lessons from nature. Vaccine 28: C14-C24. doi: 10.1016/j.vaccine.2010.07.020
|
| [125] |
Levin Y, Kochba E, Shukarev G, et al. (2016) A phase 1, open-label, randomized study to compare the immunogenicity and safety of different administration routes and doses of virosomal influenza vaccine in elderly. Vaccine 34: 5262-5272. doi: 10.1016/j.vaccine.2016.09.008
|
| [126] |
Del Giudice G, Rappuoli R, Didierlaurent AM (2018) Correlates of adjuvanticity: A review on adjuvants in licensed vaccines. Semin Immunol 39: 14-21. doi: 10.1016/j.smim.2018.05.001
|
| [127] |
Mascola JR, Fauci AS (2020) Novel vaccine technologies for the 21st century. Nat Rev Immunol 20: 87-88. doi: 10.1038/s41577-019-0243-3
|
| [128] |
Tregoning JS, Russell RF, Kinnear E (2018) Adjuvanted influenza vaccines. Hum Vaccin Immunother 14: 550-564. doi: 10.1080/21645515.2017.1415684
|
| [129] | Trucchi C, Paganino C, Orsi A, et al. (2015) Influenza vaccination in the elderly: why are the overall benefits still hotly debated? J Prev Med Hyg 56: E37-E43. |
| [130] |
Bonmarin I, Belchior E, Lévy-Bruhl D (2015) Impact of influenza vaccination on mortality in the French elderly population during the 2000–2009 period. Vaccine 33: 1099-1101. doi: 10.1016/j.vaccine.2015.01.023
|
| [131] | Koldaş ZL (2017) Vaccination in the elderly population. Turk Kardiyol Dern Ars 45: 124-127. |
| [132] |
Rizzo C, Rezza G, Ricciardi W (2018) Strategies in recommending influenza vaccination in Europe and US. Hum Vaccin Immunother 14: 693-698. doi: 10.1080/21645515.2017.1367463
|
| [133] | Triglav TK, Poljak M (2013) Vaccination indications and limits in the elderly. Acta Dermatovenerol Alp Pannonica Adriat 22: 65-70. |
| [134] |
Cano Gutierrez C, Reyes-Ortiz C, Borda MG, et al. (2016) Self-reported vaccination in the elderly: SABE Bogota study, Colombia. Colomb Med (Cali) 47: 25-30. doi: 10.25100/cm.v47i1.2107
|
| [135] |
Zeevat F, van der Schans J, Boersma WG, et al. (2019) Cost-effectiveness analysis on elderly pneumococcal vaccination in the Netherlands: Challenging the Dutch Health Council's advice. Vaccine 37: 6282-6284. doi: 10.1016/j.vaccine.2019.08.051
|
| [136] |
Naito T, Yokokawa H, Watanabe A (2018) Impact of the national routine vaccination program on 23-valent pneumococcal polysaccharide vaccine vaccination rates in elderly persons in Japan. J Infect Chemother 24: 496-498. doi: 10.1016/j.jiac.2018.01.004
|
| [137] | Domínguez A, Soldevila N, Toledo D, et al. (2016) Project Pi12/02079 Working Group. Factors associated with pneumococcal polysaccharide vaccination of the elderly in Spain: A cross-sectional study. Hum Vaccin Immunother 12: 1891-1899. |
| [138] |
Francisco PM, Borim FS, Neri AL (2015) Vaccination against influenza in the elderly: data from FIBRA, Campinas, São Paulo, Brazil. Cien Saude Colet 20: 3775-3786. doi: 10.1590/1413-812320152012.19702014
|
| [139] |
Forstner C, Kwetkat A, Schleenvoigt B, et al. (2018) Risikoimpfungen im Alter [Vaccinations in the elderly - who, when and which vaccine to use]. MMW Fortschr Med 160: 52-61. doi: 10.1007/s15006-018-0029-8
|
| [140] |
Norton EB (2019) Altered responses to pneumococcal vaccination in an elderly diabetic Japanese vaccine trial: The risk of concurrent vaccination strategies. J Diabetes Complications 33: 189-190. doi: 10.1016/j.jdiacomp.2018.12.007
|
| [141] |
Kajikawa N, Kataoka Y, Goto R, et al. (2019) Factors associated with influenza vaccination in Japanese elderly outpatients. Infect Dis Health 24: 212-221. doi: 10.1016/j.idh.2019.07.002
|
| [142] |
de Boer PT, Pouwels KB, Cox JM, et al. (2013) Cost-effectiveness of vaccination of the elderly against herpes zoster in The Netherlands. Vaccine 31: 1276-1283. doi: 10.1016/j.vaccine.2012.12.067
|
| [143] |
Paccalin M, Weinberger B, Nicolas JF, et al. (2010) The intradermal vaccination route—an attractive opportunity for influenza vaccination in the elderly. Eur Geriatr Med 1: 82-87. doi: 10.1016/j.eurger.2010.03.004
|
| [144] |
Wang J, Peng Y, Xu H, et al. (2020) The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech 21: 225. doi: 10.1208/s12249-020-01744-7
|
| [145] |
Escobar LE, Molina-Cruz A, Barillas-Mury C (2020) BCG vaccine protection from severe coronavirus disease 2019 (COVID-19). Proc Natl Acad Sci USA 117: 17720-17726. doi: 10.1073/pnas.2008410117
|
| [146] |
Kim YC, Park JH, Prausnitz MR (2012) Microneedles for drug and vaccine delivery. Adv Drug Deliv Rev 64: 1547-1568. doi: 10.1016/j.addr.2012.04.005
|
| [147] |
Zhang L, Wang W, Wang S (2015) Effect of vaccine administration modality on immunogenicity and efficacy. Expert Rev Vaccines 14: 1509-1523. doi: 10.1586/14760584.2015.1081067
|
| [148] |
Forster AH, Witham K, Depelsenaire ACI, et al. (2020) Safety, tolerability, and immunogenicity of influenza vaccination with a high-density microarray patch: Results from a randomized, controlled phase I clinical trial. PLoS Med 17: e1003024. doi: 10.1371/journal.pmed.1003024
|
| [149] |
Rouphael NG, Paine M, Mosley R, et al. (2017) TIV-MNP 2015 Study Group. The safety, immunogenicity, and acceptability of inactivated influenza vaccine delivered by microneedle patch (TIV-MNP 2015): a randomised, partly blinded, placebo-controlled, phase 1 trial. Lancet 390: 649-658. doi: 10.1016/S0140-6736(17)30575-5
|
| [150] |
Korkmaz E, Balmert SC, Sumpter TL, et al. (2021) Microarray patches enable the development of skin-targeted vaccines against COVID-19. Adv Drug Deliv Rev 171: 164-186. doi: 10.1016/j.addr.2021.01.022
|
| [151] |
Nguyen TT, Oh Y, Kim Y, et al. (2021) Progress in microneedle array patch (MAP) for vaccine delivery. Hum Vaccin Immunother 17: 316-327. doi: 10.1080/21645515.2020.1767997
|
| [152] |
Hossain MK, Ahmed T, Bhusal P, et al. (2020) Microneedle Systems for Vaccine Delivery: the story so far. Expert Rev Vaccines 19: 1153-1166. doi: 10.1080/14760584.2020.1874928
|
| [153] | Weinberger B (2020) Vaccines for Older Adults: Current Practices and Future Opportunities. Interdiscip Top Gerontol Geriatr. Basel Karger 43: VI-IX. |
| [154] | Costa R, Castagna A, Ruotolo G (2021) COVID-19 and cardiovascular problems in elderly patients: Food for thought. Aging Med (Milton) 28: 10.1002/agm2.12149. |
| [155] |
Napoli C, Tritto I, Benincasa G, et al. (2020) Cardiovascular involvement during COVID-19 and clinical implications in elderly patients. A review. Ann Med Surg (Lond) 57: 236-243. doi: 10.1016/j.amsu.2020.07.054
|
| [156] |
O'Neill LAJ, Netea MG (2020) BCG-induced trained immunity: can it offer protection against COVID-19? Nat Rev Immunol 20: 335-337. doi: 10.1038/s41577-020-0337-y
|
| [157] | European Commission I-MOVE+ Integrated Monitoring of Vaccines Effects in Europe: a platform to measure and compare effectiveness and impact of influenza and pneumococcal vaccines and vaccination strategies in the elderly Available from: https://cordis.europa.eu/project/id/634446. |
| [158] | European Centre for Disease Prevention and Control Generic protocol on enhanced surveillance for invasive pneumococcal disease at the EU/EEA level. Stockholm: ECDC Available from: https://www.ecdc.europa.eu/sites/default/files/documents/SpIDnet_Protocol_enhanced_surveillance-2018.pdf. |
| [159] |
Dirmesropian S, Wood JG, MacIntyre CR, et al. (2016) Economic Evaluation of Vaccination Programmes in Older Adults and the Elderly: Important Issues and Challenges. Pharmacoeconomics 34: 723-731. doi: 10.1007/s40273-016-0393-0
|
| [160] |
Gilbert SC (2012) T-cell-inducing vaccines—what's the future. Immunology 135: 19-26. doi: 10.1111/j.1365-2567.2011.03517.x
|
| [161] |
Ewer KJ, Barrett JR, Belij-Rammerstorfer S, et al. (2021) T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat Med 27: 270-278. doi: 10.1038/s41591-020-01194-5
|
| [162] |
van Marum RJ (2020) Underrepresentation of the elderly in clinical trials, time for action. Br J Clin Pharmacol 86: 2014-2016. doi: 10.1111/bcp.14539
|
Figures(2) / Tables(3)

Boris G Andryukov, Natalya N Besednova. Older adults: panoramic view on the COVID-19 vaccination[J]. AIMS Public Health, 2021, 8(3): 388-415. doi: 10.3934/publichealth.2021030







 DownLoad:
DownLoad: