Citation: Elspeth Molony, Christine Duncan. Income, Wealth and Health Inequalities — A Scottish Social Justice Perspective[J]. AIMS Public Health, 2016, 3(2): 255-264. doi: 10.3934/publichealth.2016.2.255

| [1] | Scottish Government Income Inequality Briefing, September 2015 http://www.gov.scot/Topics/Statistics/Browse/Social-Welfare/IncomePoverty/incomeinequalitysept2015 |
| [2] | Wilkinson R, Pickett K. The Spirit Level: why more equal societies almost always do better. London: Allen Lane; 2009. |
| [3] | Beeston C, McCartney G, Ford J, Wimbush E, Beck S, MacDonald W, et al. Health Inequalities Policy review for the Scottish Ministerial Task Force on Health Inequalities. Edinburgh: NHS Health Scotland, 2013. |
| [4] | John Rawls. A Theory of Justice. 1971 |
| [5] | The International Forum for Social Development, Department of Economic and Social Affairs, Division for Social Policy and Development. 2006 "Social Justice in an Open World: The Role of the United Nations", New York: United Nations. |
| [6] | NHS Health Scotland 2014. The Right to Health: Tackling Inequalities. http://www.healthscotland.com/documents/24729.aspx |
| [7] | Graham H., Understanding Health Inequalities. Open University Press. 2009 |
| [8] | Scottish Government., Long-term monitoring of health inequalities Headline indicators - October 2010. Edinburgh, 2010 http://www.gov.scot/Resource/Doc/328340/0106137.pdf |
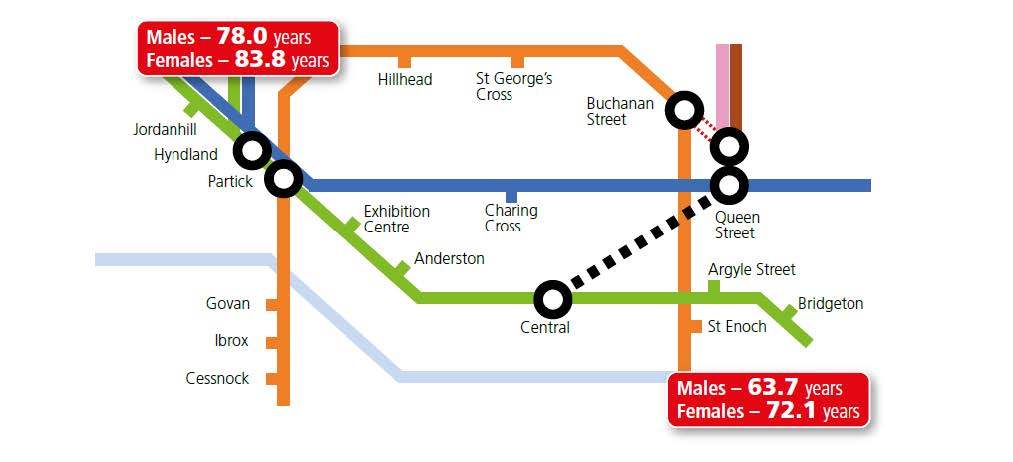
| [9] | McCartney G. Illustrating Glasgow’s health inequalities. JECH 2010; doi 10.1136/ jech.2010.120451. |
| [10] | These data have been updated using the ScotPHO profiles published in June 2015 comparing the intermediate zones – Broomhill in Glasgow’s west end (close to Jordanhill Station) and Parkhead & Barrowfield in the east end (close to Bridgeton Station). |
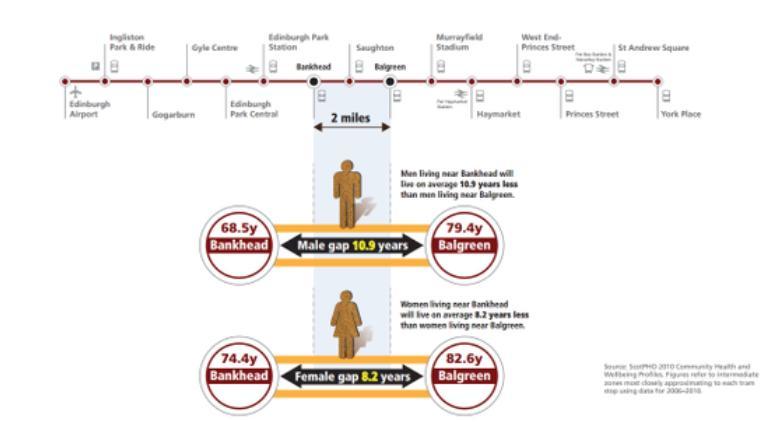
| [11] | McAuley A, McCartney G, Jones,C. Health Scotland (2015). Mind the GAP: inequalities in life expectancy in Edinburgh. http://www.healthscotland.com/documents/25059.aspx |
| [12] | NHS Health Scotland. Inequality Briefing 1: Health Inequalities – What are they? How do we reduce them? Edinburgh: NHS Health Scotland; 2015. http://www.healthscotland.com/documents/25780.aspx |
| [13] | Thomas B, Dorling D, Smith GD., Inequalities in premature mortality in Britain: observational study from 1921 to 2007., BMJ 2010;341:c3639 doi:10.1136/bmj.c3639 |
| [14] | WHO Commission on Social Determinants of Health, Closing the gap in a generation http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf |
| [15] | http://www.who.int/mediacentre/factsheets/fs323/en/ |
| [16] | Constitution of the World Health Organisation (1946) as amended, http://apps.who.int/gb/bd/PDF/bd47/EN/basic-documents-47-en.pdf |
| [17] | The Universal Declaration of Human Rights, Article 25 (1) states that ‘everyone has the right to a standard of living adequate for the health and well-being of himself and his family’, International Covenant on Economic, Social and Cultural Rights, Article 12 guarantees the right of everyone to the enjoyment of the highest attainable standard of physical and mental health. |
| [18] | Universal Declaration of Human Rights http://www.un.org/en/universal-declaration-human-rights/ |
| [19] | Economic Covenant on Economic, Social and cultural Rights http://www.ohchr.org/EN/ProfessionalInterest/Pages/CESCR.aspx |
| [20] | UN Committee on Economic, Social and Cultural Rights. 2000. General Comment on the Right to Health. |
| [21] | Commission on Social Determinants of Health. Closing the gap in a generation: Health equity through action on the social determinants of health. Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organization; 2008. |
| [22] | ScotPHO. Making a bad situation worse? The impact of welfare reform and the economic recession on health and health inequalities in Scotland (baseline report) October 2013 http://www.scotpho.org.uk/downloads/scotphoreports/scotpho131002_impactofwelfarereform_1.pdf |
| [23] | Power C, Matthews S. Origins of health inequalities in a national population sample. The Lancet. 1997; 350(9091): 1584–1589. |
| [24] | Macintyre S. The Black report and beyond what are the issues? Social Science and Medicine. 1997; 44(6): 723–745. |
| [25] | The American Heritage Dictionary of the English Language, 4th ed. Houghton Mifflin Company. Retrieved 26th November 2015 |
| [26] | http://www.gov.scot/About/Performance/scotPerforms/purposes |
| [27] | http://www.gov.scot/Topics/Statistics/Browse/Social-Welfare/IncomePoverty |
| [28] | J N Morris, A J M Donkin, D Wonderling, P Wilkinson, E A Dowler. A minimum income for healthy living. Journal of Epidemiol Community Health 2000;54:885-889 doi:10.1136/jech.54.12.885 |
| [29] | Morris JN, Wilkinson P, Dangour AD, Deeming C, Fletcher A. Defining a Minimum Income for Healthy Living: older age, England. International Journal of Epidemiology. 2007: 36 (6): 1300-7 |
| [30] | Scottish Government. Poverty and Income Inequality in Scotland: 2013/14. Edinburgh: Scottish Government; 2015. |
| [31] | Scottish Government. Additional analysis of poverty in Scotland 2013/14. Edinburgh: Scottish Government; 2015. |
| [32] | Scottish Household Survey 2013. |
| [33] | Marmot, Michael. The Health Gap: The Challenge of an Unequal World. 2015 |
| [34] | Scottish Government 2015. Public Attitudes to Poverty, Inequality and Welfare in Scotland and Britain http://www.gov.scot/Resource/0047/00473561.pdf |
| [35] | Poverty and Social Exclusion in the UK Project. Attitudes to necessities in the PSE 2012 survey: are minimum standards becoming less generous? |
| [36] | www.fairer.scot |
| [37] | www.healthier.scot |
| [38] | http://fairer.scot/2015/09/18/people-with-multiple-sclerosis-say-the-benefits-system-is-harming-their-health/ |
| [39] | http://healthier.scot/2015/09/09/why-a-fairer-scotland-would-be-a-healthier-scotland/ |
| [40] | WHO Commission on Social Determinants of Health, Closing the gap in a generation http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf |
| [41] | A Fairer Healthier Scotland, NHS Health Scotland 2012. http://www.healthscotland.com/documents/5792.aspx |

Figures(5)

Elspeth Molony, Christine Duncan. Income, Wealth and Health Inequalities — A Scottish Social Justice Perspective[J]. AIMS Public Health, 2016, 3(2): 255-264. doi: 10.3934/publichealth.2016.2.255







 DownLoad:
DownLoad: