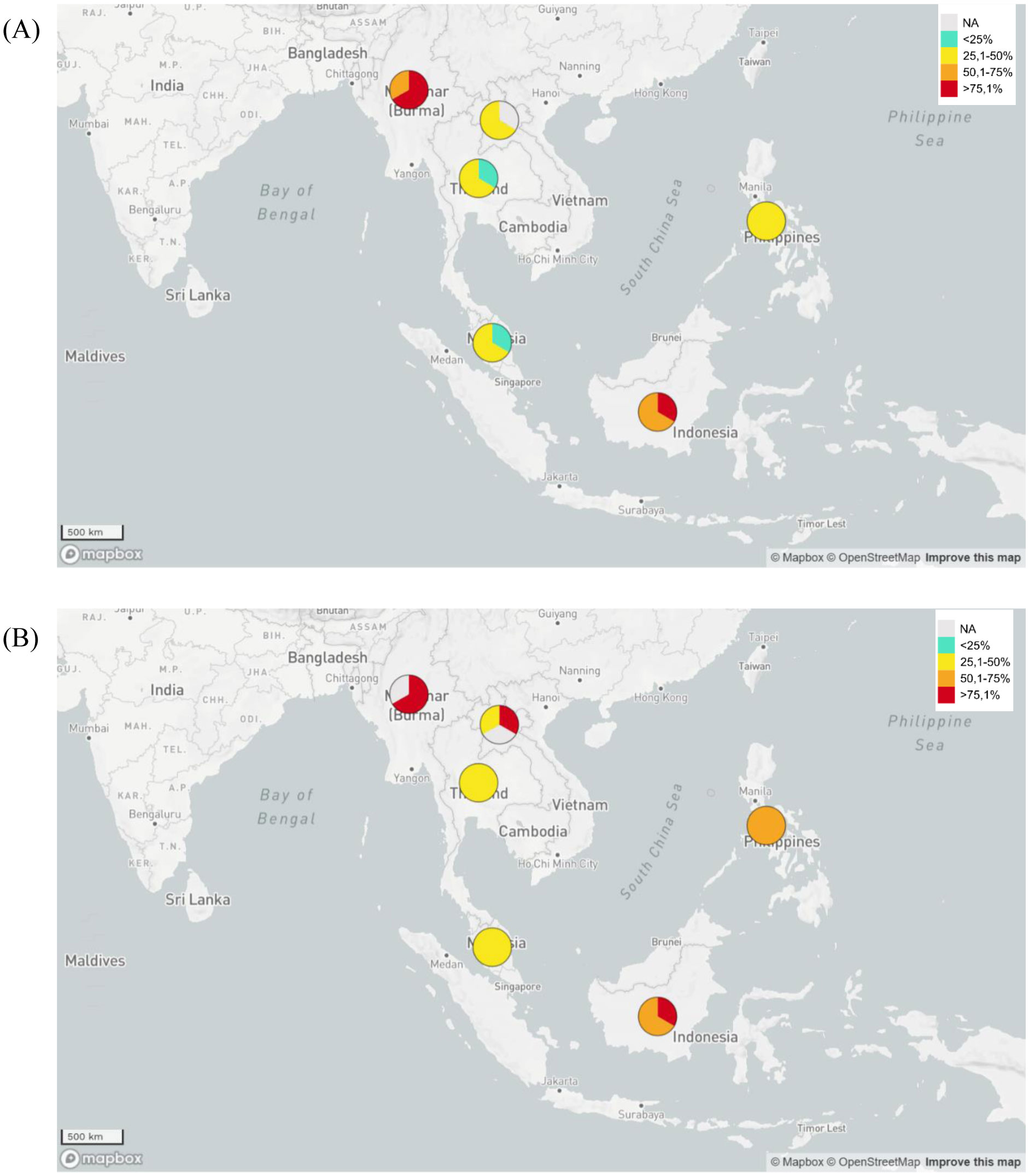
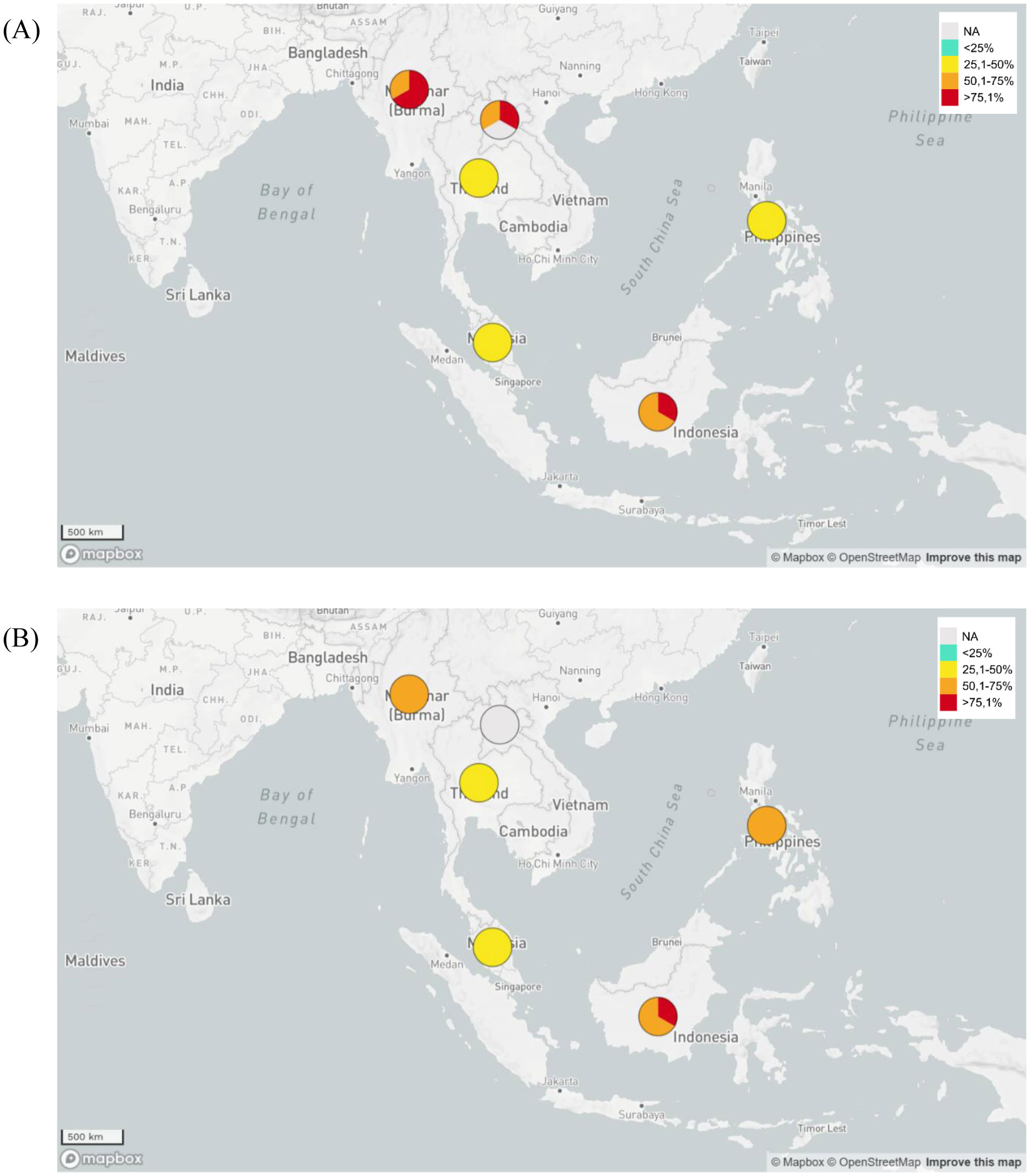
Antimicrobial resistance is the rising global health issue that should not be ignored. This problem needs to be addressed and professionally handled since it is starting to threaten global health, which eventually could lead to disaster. Extended spectrum beta lactamase (ESBL)-producing bacteria were found threatening lives, since most antibiotics were found to not be effective in treating patients with infections caused by those bacteria. ESBL-producing Escherichia coli and Klebsiella pneumoniae are the two most reported bacteria in causing the bacteremia and nosocomial infections worldwide. In this article, the prevalence of ESBL-producing E. coli and K. pneumoniae in causing blood stream and urinary tract infections in Indonesia were compared to the neighboring countries based on the global antimicrobial resistance surveillance system performed worldwide by World Health Organization (WHO). In this article, the prevalence of ESBL-producing E. coli and K. pneumoniae in Indonesia and its neighboring countries were assayed and compared in order to evaluate the antimicrobial resistances. By comparing the prevalence data to the neighboring countries, some insightful evidence and information was served to support improved health in Indonesia. Some hurdles and strategies in combating the antimicrobial resistances were further discussed. Eventually, an alternate solution to overcome the antimicrobial drug resistance should be well-provided, studied and implemented globally.
Citation: Sunarno Sunarno, Nelly Puspandari, Fitriana Fitriana, Uly Alfi Nikmah, Hasta Handayani Idrus, Novaria Sari Dewi Panjaitan. Extended spectrum beta lactamase (ESBL)-producing Escherichia coli and Klebsiella pneumoniae in Indonesia and South East Asian countries: GLASS Data 2018[J]. AIMS Microbiology, 2023, 9(2): 218-227. doi: 10.3934/microbiol.2023013
Antimicrobial resistance is the rising global health issue that should not be ignored. This problem needs to be addressed and professionally handled since it is starting to threaten global health, which eventually could lead to disaster. Extended spectrum beta lactamase (ESBL)-producing bacteria were found threatening lives, since most antibiotics were found to not be effective in treating patients with infections caused by those bacteria. ESBL-producing Escherichia coli and Klebsiella pneumoniae are the two most reported bacteria in causing the bacteremia and nosocomial infections worldwide. In this article, the prevalence of ESBL-producing E. coli and K. pneumoniae in causing blood stream and urinary tract infections in Indonesia were compared to the neighboring countries based on the global antimicrobial resistance surveillance system performed worldwide by World Health Organization (WHO). In this article, the prevalence of ESBL-producing E. coli and K. pneumoniae in Indonesia and its neighboring countries were assayed and compared in order to evaluate the antimicrobial resistances. By comparing the prevalence data to the neighboring countries, some insightful evidence and information was served to support improved health in Indonesia. Some hurdles and strategies in combating the antimicrobial resistances were further discussed. Eventually, an alternate solution to overcome the antimicrobial drug resistance should be well-provided, studied and implemented globally.

| [1] |
Ferri M, Ranucci E, Romagnoli P, et al. (2017) Antimicrobial resistance: a global emerging threat to public health systems. Crit Rev Food Sci Nutr 57: 2857-2876. https://doi.org/10.1080/10408398.2015.1077192 
|
| [2] | O'Neill J Tackling drug-resistant infections globally: final report and recommendations (2016). |
| [3] | (2016) World BankDrug-resistant infections: a threat to our economic future. Washington: The World Bank Group. |
| [4] | Matsumoto H, Komiya K, Ichihara S, et al. (2022) Factors associated with extended-spectrum β-lactamase-producing Enterobacteria isolated from respiratory samples. Int Med . https://doi.org/10.2169/internalmedicine.0690-22 |
| [5] |
Panjaitan NSD, Lestari CSW (2022) A response to research article “cefmetazole resistance mechanism for Escherichia Coli including ESBL-producing strains”. Infect Drug Resist 15: 6065-6066. https://doi.org/10.1371/journal.pone.0201688
|
| [6] |
Malchione MD, Torres LM, Hartley DM, et al. (2019) Carbapenem and colistin resistance in Enterobacteriaceae in Southeast Asia: review and mapping of emerging and overlapping challenges. Int J Antimicrob Agents 54: 381-399. https://doi.org/10.1016/j.ijantimicag.2019.07.019
|
| [7] |
Ghasemian A, Shafiei M, Hasanvand F, et al. (2018) Carbapenem and colistin resistance in Enterobacteriaceae: worldwide spread and future perspectives. Rev Res Med Microbiol 29: 173-176. https://doi.org/10.1097/MRM.0000000000000142
|
| [8] |
Alaoui Mdarhri H, Benmessaoud R, Yacoubi H, et al. (2022) Alternatives therapeutic approaches to conventional antibiotics: advantages, limitations and potential application in medicine. Antibiotics 11: 1826. https://doi.org/10.3390/antibiotics11121826
|
| [9] |
Zyman A, Górski A, Międzybrodzki R (2022) Phage therapy of wound-associated infections. Folia Microbiol 67: 193-201. https://doi.org/10.1007/s12223-021-00946-1
|
| [10] | World Health OrganizationGlobal action plan on antimicrobial resistance (2015). Available from: https://www.who.int/publications/i/item/9789241509763 |
| [11] | White House AdministrationNational Action Plan for Combating Antibiotic-Resistant Bacteria (2015). Available from: https://www.cdc.gov/drugresistance/pdf/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf |
| [12] | Ministry of Health Republic of IndonesiaNational Action Plan on Antimicrobial Resistance Indonesia 2017–2019 (2017). Available from: https://www.who.int/publications/m/item/indonesia-national-action-plan-on-antimicrobial-resistance-indonesia-2017-2019 |
| [13] |
Saliba R, Zahar JR, Dabar G, et al. (2023) Limiting the spread of multidrug-resistant bacteria in low-to-middle-income countries: one size does not fit all. Pathogens 12: 144. https://doi.org/10.3390/pathogens12010144
|
| [14] |
Sharma A, Luvsansharav UO, Paul P, et al. (2021) Multi-country cross-sectional study of colonization with multidrug-resistant organisms: protocol and methods for the Antibiotic Resistance in Communities and Hospitals (ARCH) studies. BMC Public Health 21: 1-9. https://doi.org/10.1186/s12889-021-11451-y
|
| [15] |
Tornimbene B, Eremin S, Escher M, et al. (2018) WHO global antimicrobial resistance surveillance system early implementation 2016-17. Lancet Infect Dis 18: 241-242. https://doi.org/10.1016/S1473-3099(18)30060-4
|
| [16] |
Puspandari N, Sunarno S, Febrianti T, et al. (2021) Extended spectrum beta-lactamase-producing Escherichia coli surveillance in the human, food chain, and environment sectors: Tricycle project (pilot) in Indonesia. One Health 13: 100331. https://doi.org/10.1016/j.onehlt.2021.100331
|
| [17] | World Health OrganizationGLASS Country, territory and area profiles (2018). Available from: https://apps.who.int/gho/tableau-public/tpc-frame.jsp?id=2012 |
| [18] |
Kaper JB, Nataro JP, Mobley HLT (2004) Pathogenic escherichia coli. Nat Rev Microbiol 2: 123-140. https://doi.org/10.1038/nrmicro818
|
| [19] |
Uslan DZ, Crane SJ, Steckelberg JM, et al. (2007) Age-and sex-associated trends in bloodstream infection: a population-based study in Olmsted County, Minnesota. Arch Intern Med 167: 834-839. https://doi.org/10.1001/archinte.167.8.834
|
| [20] |
Kim YC, Choi H, Kim YA, et al. (2023) Risk factors and microbiological features of recurrent Escherichia coli bloodstream infections. PLoS One 18: e0280196. https://doi.org/10.1371/journal.pone.0280196
|
| [21] |
Yamasaki S, Shigemura K, Osawa K, et al. (2021) Genetic analysis of ESBL-producing Klebsiella pneumoniae isolated from UTI patients in Indonesia. J Infect Chemother 27: 55-61. https://doi.org/10.1016/j.jiac.2020.08.007
|
| [22] |
Panjaitan NSD, Horng YT, Cheng SW, et al. (2019) EtcABC, a putative EII complex, regulates type 3 fimbriae via CRP-cAMP signaling in Klebsiella pneumoniae. Front Microbiol 10: 1558. https://doi.org/10.3389/fmicb.2019.01558
|
| [23] |
Schaufler K, Nowak K, Düx A, et al. (2018) Clinically relevant ESBL-producing K. pneumoniae ST307 and E. coli ST38 in an urban West African rat population. Front Microbiol 9: 150. https://doi.org/10.3389/fmicb.2018.00150
|
| [24] |
Botelho J, Cazares A, Schulenburg H (2023) The ESKAPE mobilome contributes to the spread of antimicrobial resistance and CRISPR-mediated conflict between mobile genetic elements. Nucleic Acids Res 51: 236-252. https://doi.org/10.1093/nar/gkac1220
|
| [25] | Uchil RR, Kohli GS, KateKhaye VM, et al. (2014) Strategies to combat antimicrobial resistance. J Clin Diagn Res 8: ME01-ME04. https://doi.org/10.7860/JCDR/2014/8925.4529 |
| [26] |
Inoue H (2019) Strategic approach for combating antimicrobial resistance (AMR). Global Health Med 1: 61-64. https://doi.org/10.35772/ghm.2019.01026
|
| [27] | Eleraky NE, Allam A, Hassan SB, et al. (2020) Nanomedicine fight against antibacterial resistance: an overview of the recent pharmaceutical innovations. Pharm 12: 142. https://doi.org/10.3390/pharmaceutics12020142 |
| [28] |
Bunse M, Daniels R, Gründemann C, et al. (2022) Essential oils as multicomponent mixtures and their potential for human health and well-being. Front Pharmacol 13. https://doi.org/10.3389/fphar.2022.956541
|
| [29] |
Badescu B, Buda V, Romanescu M, et al. (2022) Current state of knowledge regarding WHO critical priority pathogens: Mechanisms of resistance and proposed solutions through candidates such as essential oils. Plants 11: 1789. https://doi.org/10.3390/plants11141789
|
| [30] |
Iubatti M, Gabas IM, Cavaco LM, et al. (2022) Antisense peptide nucleic acid–diaminobutanoic acid dendron conjugates with sbma-independent antimicrobial activity against gram-negative bacteria. ACS Infect Dis 8: 1098-1106. https://doi.org/10.1021/acsinfecdis.2c00089
|
| [31] | Matzaras R, Nikopoulou A, Protonotariou E, et al. (2022) Gut microbiota modulation and prevention of dysbiosis as an alternative approach to antimicrobial resistance: a narrative review. Yale J Biol Med 95: 479-494. |
| [32] |
Ianiro G, Punčochář M, Karcher N, et al. (2022) Variability of strain engraftment and predictability of microbiome composition after fecal microbiota transplantation across different diseases. Nat Med 28: 1913-1923. https://doi.org/10.1038/s41591-022-01964-3
|
| [33] | Ministry of Health MalaysiaMalaysian Action Plan on Antimicrobial Resistance (MyAP-AMR) 2017–2021 (2017). Available from: https://faolex.fao.org/docs/pdf/mal189905.pdf |
Figures(2) / Tables(1)

Sunarno Sunarno, Nelly Puspandari, Fitriana Fitriana, Uly Alfi Nikmah, Hasta Handayani Idrus, Novaria Sari Dewi Panjaitan. Extended spectrum beta lactamase (ESBL)-producing Escherichia coli and Klebsiella pneumoniae in Indonesia and South East Asian countries: GLASS Data 2018[J]. AIMS Microbiology, 2023, 9(2): 218-227. doi: 10.3934/microbiol.2023013







 DownLoad:
DownLoad: