Fall is the most common patient safety incident in health care organizations. This study was initiated to obtain information regarding knowledge & attitude on falls and awareness of fall risk factors among nurses to device evidence-based and multidisciplinary educational and training programs to improve patient safety and thereby reduce morbidity and mortality associated with falls.
A descriptive cross-sectional survey study was conducted among 339 registered nurses working in Tertiary care hospitals across Chennai, Tamil Nadu, India. A modified version of the previously validated standard questionnaire was administered by the investigators through an online survey method to explore the level of knowledge & attitude on falls and awareness of inpatient fall risk factors among Nurses.
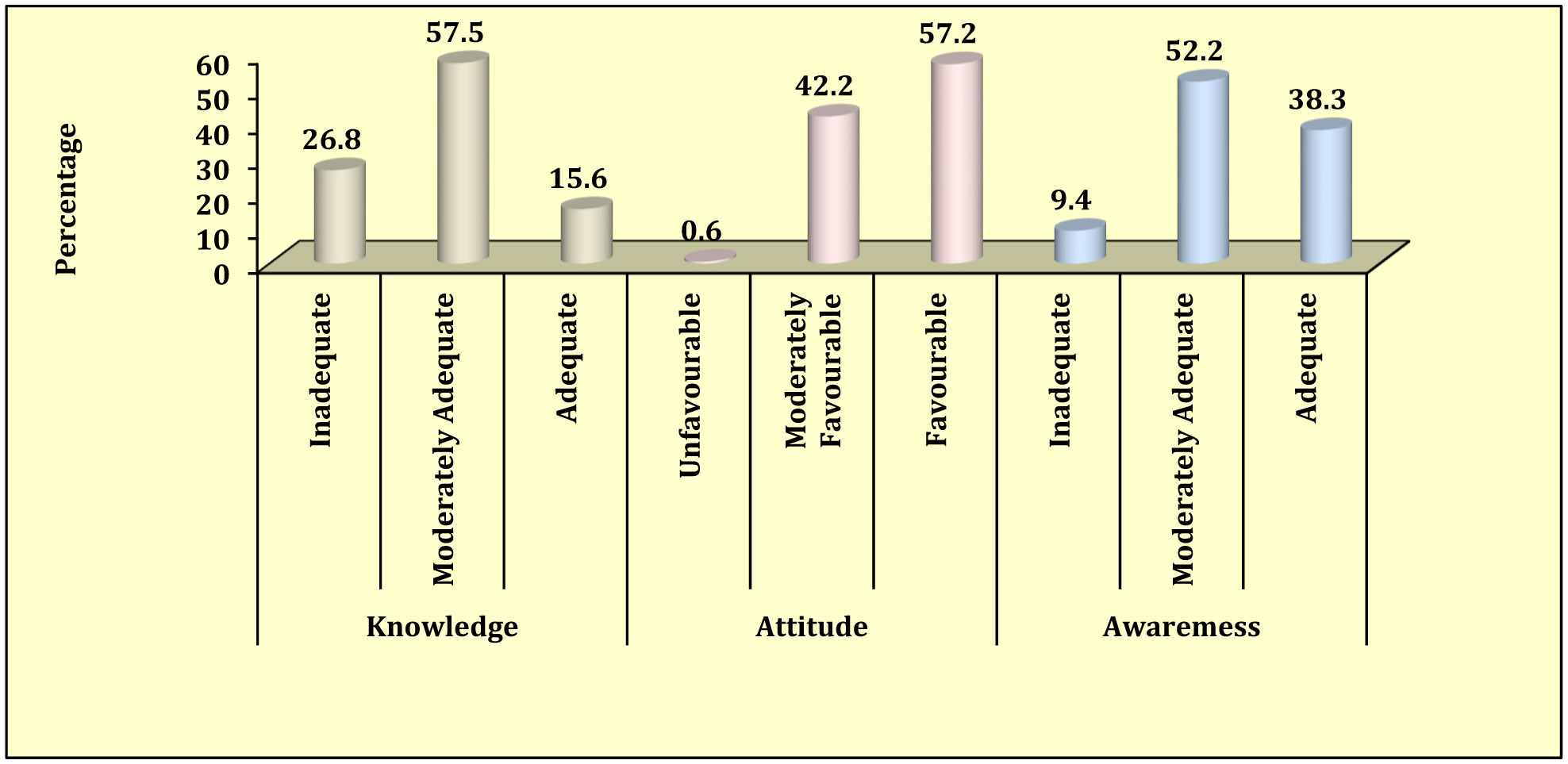
In this study, 15.6% of participants had adequate knowledge of falls, 57.2% had a favorable attitude towards falls and 38.3% had adequate awareness of fall risk factors. Years of experience in nursing has a statistically significant association with the level of knowledge on fall. The participant's attitude towards falls had a statistically significant relationship with age, education, experience in nursing, and previous patient fall experience. The correlation between fall knowledge, the attitude toward falls, and awareness of fall risk factors were highly significant. The majority of the participants expressed their favorable attitude toward the need for fall preventive education.
In our study, it is evident that there is a void that has to be filled to improve the knowledge, attitude, and awareness of falls and their risk factors. There is a need for extensive education and holistic, multifactorial, and interdisciplinary training program to be undertaken through various health care organizations.
Citation: Kavin Mozhi James, Divya Ravikumar, Sindhura Myneni, Poonguzhali Sivagananam, Poongodi Chellapandian, Rejili Grace Joy Manickaraj, Yuvasree Sargunan, Sai Ravi Teja Kamineni, Vishnu Priya Veeraraghavan, Malathi Kullappan, Surapaneni Krishna Mohan. Knowledge, attitudes on falls and awareness of hospitalized patient's fall risk factors among the nurses working in Tertiary Care Hospitals[J]. AIMS Medical Science, 2022, 9(2): 304-321. doi: 10.3934/medsci.2022013
Fall is the most common patient safety incident in health care organizations. This study was initiated to obtain information regarding knowledge & attitude on falls and awareness of fall risk factors among nurses to device evidence-based and multidisciplinary educational and training programs to improve patient safety and thereby reduce morbidity and mortality associated with falls.
A descriptive cross-sectional survey study was conducted among 339 registered nurses working in Tertiary care hospitals across Chennai, Tamil Nadu, India. A modified version of the previously validated standard questionnaire was administered by the investigators through an online survey method to explore the level of knowledge & attitude on falls and awareness of inpatient fall risk factors among Nurses.
In this study, 15.6% of participants had adequate knowledge of falls, 57.2% had a favorable attitude towards falls and 38.3% had adequate awareness of fall risk factors. Years of experience in nursing has a statistically significant association with the level of knowledge on fall. The participant's attitude towards falls had a statistically significant relationship with age, education, experience in nursing, and previous patient fall experience. The correlation between fall knowledge, the attitude toward falls, and awareness of fall risk factors were highly significant. The majority of the participants expressed their favorable attitude toward the need for fall preventive education.
In our study, it is evident that there is a void that has to be filled to improve the knowledge, attitude, and awareness of falls and their risk factors. There is a need for extensive education and holistic, multifactorial, and interdisciplinary training program to be undertaken through various health care organizations.

| [1] |
Lamb SE, Jørstad-Stein EC, Hauer K, et al. (2005) Development of a common outcome data set for fall injury prevention trials: the Prevention of Falls Network Europe consensus. J Am Geriatr Soc 53: 1618-1622. https://doi.org/10.1111/j.1532-5415.2005.53455.x 
|
| [2] | World Health OrganizationThe global burden of disease: 2004 update (2008). Available from: https://apps.who.int/iris/handle/10665/43942 |
| [3] |
Healey F, Darowski A (2012) Older patients and falls in hospital. Clin Risk 18: 170-176. https://doi.org/10.1258/cr.2012.012020
|
| [4] | Healey FM (2011) The prevention of patient falls in healthcare settings, with particular emphasis on the effect of bedrail use on falls and injury as part of multi-faceted interventions. Doctoral dissertation, Newcastle University . |
| [5] | Kumar A, Srivastava DK, Verma A, et al. (2013) The problems of fall, risk factors and their management among geriatric population in India. Indian J Community Health 25: 89-94. |
| [6] | Dsouza SA, Rajashekar B, Dsouza HS, et al. (2014) Falls in Indian older adults: a barrier to active ageing. Asian J Gerontol Geriatr 9: 33-40. |
| [7] |
Williams JS, Kowal P, Hestekin H, et al. (2015) Prevalence, risk factors and disability associated with fall-related injury in older adults in low- and middle-incomecountries: results from the WHO Study on global AGEing and adult health (SAGE). BMC Med 13: 147. https://doi.org/10.1186/s12916-015-0390-8
|
| [8] | World Health OrganizationAgeing, Life Course Unit. WHO global report on falls prevention in older age (2008). Available from: https://www.who.int/publications/i/item/9789241563536 |
| [9] |
Mitchell-Fearon K, James K, Waldron N, et al. (2014) Falls among community-dwelling older adults in Jamaica. SAGE Open 4: 2158244014564351. https://doi.org/10.1177/2158244014564351
|
| [10] |
Inouye SK, Studenski S, Tinetti ME, et al. (2007) Geriatric syndromes: clinical, research and policy implications of a core geriatric concept. J Am Geriatr Soc 55: 780-791. https://doi.org/10.1111/j.1532-5415.2007.01156.x
|
| [11] |
Smith G, Kydd A (2016) Editorial: getting care of older people right. The need for appropriate frailty assessment. J Clin Nurs 26: 5-6. https://doi.org/10.1111/jocn.13618
|
| [12] |
Tzeng HM, Yin CY (2013) Frequently observed risk factors for fall-related injuries and effective preventive interventions: a multihospital survey of nurses' perceptions. J Nurs Care Qual 28: 130-138. https://doi.org/10.1097/NCQ.0b013e3182780037
|
| [13] |
Campbell B (2016) Patient falls: preventable, not inevitable. Nurs Made Incred Easy 14: 14-18. https://doi.org/10.1097/01.NME.0000475168.08103.37
|
| [14] |
Shojania KG, Marang-van de Mheen PJ (2015) Temporal trends in patient safety in the Netherlands: reductions in preventable adverse events or the end of adverse events as a useful metric?. BMJ Qual Saf 24: 541-544. https://doi.org/10.1136/bmjqs-2015-004461
|
| [15] |
Cangany M, Back D, Hamilton-Kelly T, et al. (2015) Bedside nurses leading the way for falls prevention: an evidence-based approach. Crit Care Nurse 35: 82-84. https://doi.org/10.4037/ccn2015414
|
| [16] | Seo OI (2008) Influence of knowledge and attitude on behaviors of falls prevention activities in patient among university hospital nurse. Unpublished master's thesis, The Catholic University of Korea, Seoul . |
| [17] | Kim CG (2011) Nurses' knowledge and attitude toward fall in hospitalized patients. J Ind Sci Res 28: 275-281. |
| [18] |
Kim MH, Jeon HW, Chon MY (2015) Study on the knowledge and attitudes of falls and awareness of fall risk factors among nursing students. Indian J Sci Technol 8: 74. https://doi.org/10.17485/ijst/2015/v8iS1/57593
|
| [19] |
Laing SS, Silver IF, York S, et al. (2011) Fall prevention knowledge, attitude, and practices of community stakeholders and older adults. J Aging Res 2011. https://doi.org/10.4061/2011/395357
|
| [20] | Choi BH (2011) The nursing student's attitude and preventive activities on inpatients falls. Unpublished master's thesis, Keimyung University . |
| [21] |
Asiri F, ALMohiza MA, Faia Aseeri M, et al. (2018) Fall prevention knowledge and practice patterns among home healthcare professionals in southern Saudi Arabia: an observational study. J Int Med Res 46: 5062-5073. https://doi.org/10.1177/0300060518789816
|
| [22] | Gutta S, Joseph A, Chakraborty A, et al. (2013) Study on the knowledge, attitudes and practices regarding prevention of recurrent falls in the elderly. IOSR J Dent Med Sci 9: 32-38. https://doi.org/10.9790/0853-0933238 |
| [23] |
Kalu ME, Vlachantoni A, Norman KE (2019) Knowledge about risk factors for falls and practice about fall prevention in older adults among physiotherapists in Nigeria. Physiother Res Int 24: e1742. https://doi.org/10.1002/pri.1742
|
Figures(1) / Tables(7)

Kavin Mozhi James, Divya Ravikumar, Sindhura Myneni, Poonguzhali Sivagananam, Poongodi Chellapandian, Rejili Grace Joy Manickaraj, Yuvasree Sargunan, Sai Ravi Teja Kamineni, Vishnu Priya Veeraraghavan, Malathi Kullappan, Surapaneni Krishna Mohan. Knowledge, attitudes on falls and awareness of hospitalized patient's fall risk factors among the nurses working in Tertiary Care Hospitals[J]. AIMS Medical Science, 2022, 9(2): 304-321. doi: 10.3934/medsci.2022013







 DownLoad:
DownLoad: