Cardiac arrest (CA) is a fatal acute event. The development of new CA early warning system based on time series of vital signs from electronic health records (EHR) has great potential to reduce CA damage. In this process, recursive architecture-based deep learning, as a powerful tool for time series data processing, enables automatically extract features from various monitoring clinical parameters and to further improve the performance for acute critical illness prediction. However, the unexplainable nature and excessive time caused by black box structure with poor parallelism are the limitations of its development, especially in the CA clinical application with strict requirement of emergency treatment and low hidden dangers. In this study, we present an explainable and efficient deep early warning system for CA prediction, which features are captured by an efficient temporal convolutional network (TCN) on EHR clinical parameters sequence and explained by deep Taylor decomposition (DTD) theoretical framework. To demonstrate the feasibility of our method and further evaluate its performance, prediction and explanation experiments were performed. Experimental results show that our method achieves superior CA prediction accuracy compared with standard national early warning score (NEWS), in terms of overall AUROC (0.850 Vs. 0.476) and F1-Score (0.750 Vs. 0.450). Furthermore, our method improves the interpretability and efficiency of deep learning-based CA early warning system. It provides the relevance of prediction results for each clinical parameter and about 1.7 times speed enhancement for system calculation compared with the long short-term memory network.
Citation: Qinhua Tang, Xingxing Cen, Changqing Pan. Explainable and efficient deep early warning system for cardiac arrest prediction from electronic health records[J]. Mathematical Biosciences and Engineering, 2022, 19(10): 9825-9841. doi: 10.3934/mbe.2022457
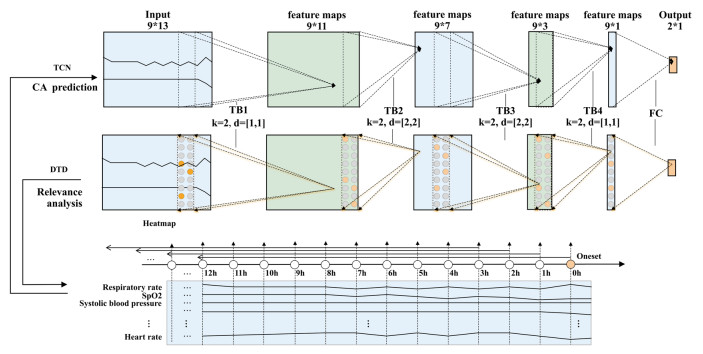
Cardiac arrest (CA) is a fatal acute event. The development of new CA early warning system based on time series of vital signs from electronic health records (EHR) has great potential to reduce CA damage. In this process, recursive architecture-based deep learning, as a powerful tool for time series data processing, enables automatically extract features from various monitoring clinical parameters and to further improve the performance for acute critical illness prediction. However, the unexplainable nature and excessive time caused by black box structure with poor parallelism are the limitations of its development, especially in the CA clinical application with strict requirement of emergency treatment and low hidden dangers. In this study, we present an explainable and efficient deep early warning system for CA prediction, which features are captured by an efficient temporal convolutional network (TCN) on EHR clinical parameters sequence and explained by deep Taylor decomposition (DTD) theoretical framework. To demonstrate the feasibility of our method and further evaluate its performance, prediction and explanation experiments were performed. Experimental results show that our method achieves superior CA prediction accuracy compared with standard national early warning score (NEWS), in terms of overall AUROC (0.850 Vs. 0.476) and F1-Score (0.750 Vs. 0.450). Furthermore, our method improves the interpretability and efficiency of deep learning-based CA early warning system. It provides the relevance of prediction results for each clinical parameter and about 1.7 times speed enhancement for system calculation compared with the long short-term memory network.

| [1] |
S. Girotra, B. K. Nallamothu, J. A. Spertus, Y. Li, H. M. Krumholz, P. S. Chan, Trends in survival after in-hospital cardiac arrest, N. Engl. J. Med., 367 (2012), 1912-1920. https://doi.org/10.1016/j.jemermed.2013.02.007 doi: 10.1016/j.jemermed.2013.02.007

|
| [2] |
L. Mandigers, F. Termorshuizen, N. F. Keizer, D. Gommers, D. Reis Miranda, W. J. Rietdijk, et al., A nationwide overview of 1-year mortality in cardiac arrest patients admitted to intensive care units in the Netherlands between 2010 and 2016, Resuscitation, 147 (2020), 88-94. https://doi.org/10.1016/j.resuscitation.2019.12.029 doi: 10.1016/j.resuscitation.2019.12.029
|
| [3] |
J. Soar, J. P. Nolan, B. W. Böttiger, G. D. Perkins, C. Lott, N. I. Nikolaou, et al., European resuscitation council guidelines for resuscitation 2015: section 3. Adult advanced life support, Resuscitation, 95 (2015), 100-147. https://doi.org/10.1016/j.resuscitation.2015.07.016 doi: 10.1016/j.resuscitation.2015.07.016
|
| [4] | G. B. Smith, D. R. Prytherch, P. Meredith, P. E. Schmidt, P. I. Featherstone, The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death, Resuscitation, 84 (2013), 465-470. https://doi.org/10.1016/j.resuscitation.2012.12.016 |
| [5] |
I. Nishijima, S. Oyadomari, S. Maedomari, R. Toma, C. Igei, S. Kobata, et al., Use of a modified early warning score system to reduce the rate of in-hospital cardiac arrest, J. Intensive Care, 4 (2016), 1-6. https://doi.org/10.1186/s40560-016-0134-7 doi: 10.1186/s40560-016-0134-7
|
| [6] |
F. E. Shamout, T. Zhu, P. Sharma, P. J. Watkinson, D. A. Clifton, Deep interpretable early warning system for the detection of clinical deterioration, IEEE J. Biomed. Heal. Inf., 24 (2019), 437-446. https://doi.org/10.1109/jbhi.2019.2937803 doi: 10.1109/jbhi.2019.2937803
|
| [7] |
J. Kwon, Y. Lee, Y. Lee, S. Lee, J. Park, An algorithm based on deep learning for predicting in‐hospital cardiac arrest, J. Am. Heart Assoc., 7 (2018), 1-11. https://doi.org/10.1161/jaha.118.008678 doi: 10.1161/jaha.118.008678
|
| [8] |
J. Kim, M. Chae, H. J. Chang, Y. A. Kim, E. Park, Predicting cardiac arrest and respiratory failure using feasible artificial intelligence with simple trajectories of patient data, J. Clin. Med., 8 (2019), 1336-1350. https://doi.org/10.3390/jcm8091336 doi: 10.3390/jcm8091336
|
| [9] |
T. Pham, T. Tran, D. Phung, S. Venkatesh, Predicting healthcare trajectories from medical records: A deep learning approach, J. Biomed. Inf., 69 (2017), 218-229. https://doi.org/10.1016/j.jbi.2017.04.001 doi: 10.1016/j.jbi.2017.04.001
|
| [10] |
S. M. Lauritsen, M. E. Kalør, E. L. Kongsgaard, K. M. Lauritsen, M. J. Jørgensen, J. Lange, et al., Early detection of sepsis utilizing deep learning on electronic health record event sequences, Artif. Intell. Med., 104 (2020), 101820. https://doi.org/10.1016/j.artmed.2020.101820 doi: 10.1016/j.artmed.2020.101820
|
| [11] | M. Aczon, D. Ledbetter, L. Ho, A. Gunny, A. Flynn, J. Williams, et al., Dynamic mortality risk predictions in pediatric critical care using recurrent neural networks, preprint, arXiv: 1701.06675. |
| [12] |
H. Harutyunyan, H. Khachatrian, D. C. Kale, G. Ver Steeg, A. Galstyan, Multitask learning and benchmarking with clinical time series data, Sci. Data, 6 (2019), 1-18. https://doi.org/10.1038/s41597-019-0103-9 doi: 10.1038/s41597-019-0103-9
|
| [13] |
S. Hong, S. Lee, J. Lee, W. Cha, K. Kim, Prediction of cardiac arrest in the emergency department based on machine learning and sequential characteristics: model development and retrospective clinical validation study, JMIR Med. Inf., 8 (2020), 1-14. https://doi.org/10.2196/15932 doi: 10.2196/15932
|
| [14] |
Y. J. Lee, K Cho, O. Kwon, H. Park, Y. Lee, J. Kwon, et al., A multicentre validation study of the deep learning-based early warning score for predicting in-hospital cardiac arrest in patients admitted to general wards, Resuscitation, 163 (2021), 78-85. https://doi.org/10.1016/j.resuscitation.2021.04.013 doi: 10.1016/j.resuscitation.2021.04.013
|
| [15] |
S. J. Park, K. Cho, O. Kwon, H. Park, Y. Lee, W. H. Shim, et al., Development and validation of a deep-learning-based pediatric early warning system: A single-center study, Biomed. J., 45 (2022), 155-168. https://doi.org/10.1016/j.bj.2021.01.003 doi: 10.1016/j.bj.2021.01.003
|
| [16] | M. Moor, M. Horn, B. Rieck, D. Roqueiro, K. Borgwardt, Temporal convolutional networks and dynamic time warping can drastically improve the early prediction of sepsis, preprint, arXiv: 1902.01659. |
| [17] | S. Bai, J. Z. Kolter, V. Koltun, An empirical evaluation of generic convolutional and recurrent networks for sequence modeling, preprint, arXiv: 1803.01271. |
| [18] | Y. Chang, J. Rubin, G. Boverman, S. Vij, A. Rahman, A. Natarajan, et al., A multi-task imputation and classification neural architecture for early prediction of sepsis from multivariate clinical time series, in 2019 Computing in Cardiology (CinC), (2019), 1-4. https://doi.org/10.23919/CinC49843.2019.9005751 |
| [19] |
N. Sato, E. Uchino, R. Kojima, S. Hiragi, M. Yanagita, Y. Okuno, Prediction and visualization of acute kidney injury in intensive care unit using one-dimensional convolutional neural networks based on routinely collected data, Comput. Methods Programs Biomed., 206 (2021), 106129. https://doi.org/10.1016/j.cmpb.2021.106129 doi: 10.1016/j.cmpb.2021.106129
|
| [20] | O. Almqvist, A comparative study between algorithms for time series forecasting on customer prediction: An investigation into the performance of ARIMA, RNN, LSTM, TCN and HMM, 2019. Available from: https://www.researchgate.net/publication/333731678 |
| [21] |
G. Montavon, S. Lapuschkin, A. Binder, W. Samek, K. R. Müller, Explaining nonlinear classification decisions with deep taylor decomposition, Pattern Recognit., 65 (2017), 211-222. https://doi.org/10.1016/j.patcog.2016.11.008 doi: 10.1016/j.patcog.2016.11.008
|
| [22] |
C. Xiao, E. Choi, J. Sun, Opportunities and challenges in developing deep learning models using electronic health records data: a systematic review, J. Am. Med. Inf. Assoc., 25 (2018), 1419-1428. https://doi.org/10.1093/jamia/ocy068 doi: 10.1093/jamia/ocy068
|
| [23] |
B. Shickel, P. J. Tighe, A. Bihorac, P. Rashidi, Deep EHR: A survey of recent advances in deep learning techniques for electronic health record (EHR) analysis, IEEE J. Biomed. Heal. Inf., 22 (2017), 1589-1604. https://doi.org/10.1109/jbhi.2017.2767063 doi: 10.1109/jbhi.2017.2767063
|
| [24] |
W. Samek, G. Montavon, S. Lapuschkin, C. J. Anders, K. R. Müller, Explaining deep neural networks and beyond: A review of methods and applications, Proc. IEEE, 109 (2021), 247-278. https://doi.org/10.1109/jproc.2021.3060483 doi: 10.1109/jproc.2021.3060483
|
| [25] | H. Chefer, S. Gur, L. Wolf, Transformer interpretability beyond attention visualization, in 2021 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), (2021), 782-791. https://doi.org/10.1109/cvpr46437.2021.00084 |
| [26] | W. J. Nam, S. Gur, J. Choi, L. Wolf, S. W. Lee, Relative attributing propagation: Interpreting the comparative contributions of individual units in deep neural networks, in Proceedings of the AAAI Conference on Artificial Intelligence, 34 (2020), 2501-2508. https://doi.org/10.1609/aaai.v34i03.5632 |
| [27] | S. Gur, A. Ali, L. Wolf, Visualization of Supervised and Self-Supervised Neural Networks via Attribution Guided Factorization, preprint, arXiv: 2012.02166. |
| [28] |
S. M. Lauritsen, M. Kristensen, M. V. Olsen, M. S. Larsen, K. M. Lauritsen, M. J. Jørgensen, et al., Explainable artificial intelligence model to predict acute critical illness from electronic health records, Nat. Commun., 11 (2020), 1-11. https://doi.org/10.1038/s41467-020-17431-x doi: 10.1038/s41467-020-17431-x
|






Figures(7) / Tables(5)

Qinhua Tang, Xingxing Cen, Changqing Pan. Explainable and efficient deep early warning system for cardiac arrest prediction from electronic health records[J]. Mathematical Biosciences and Engineering, 2022, 19(10): 9825-9841. doi: 10.3934/mbe.2022457







 DownLoad:
DownLoad: