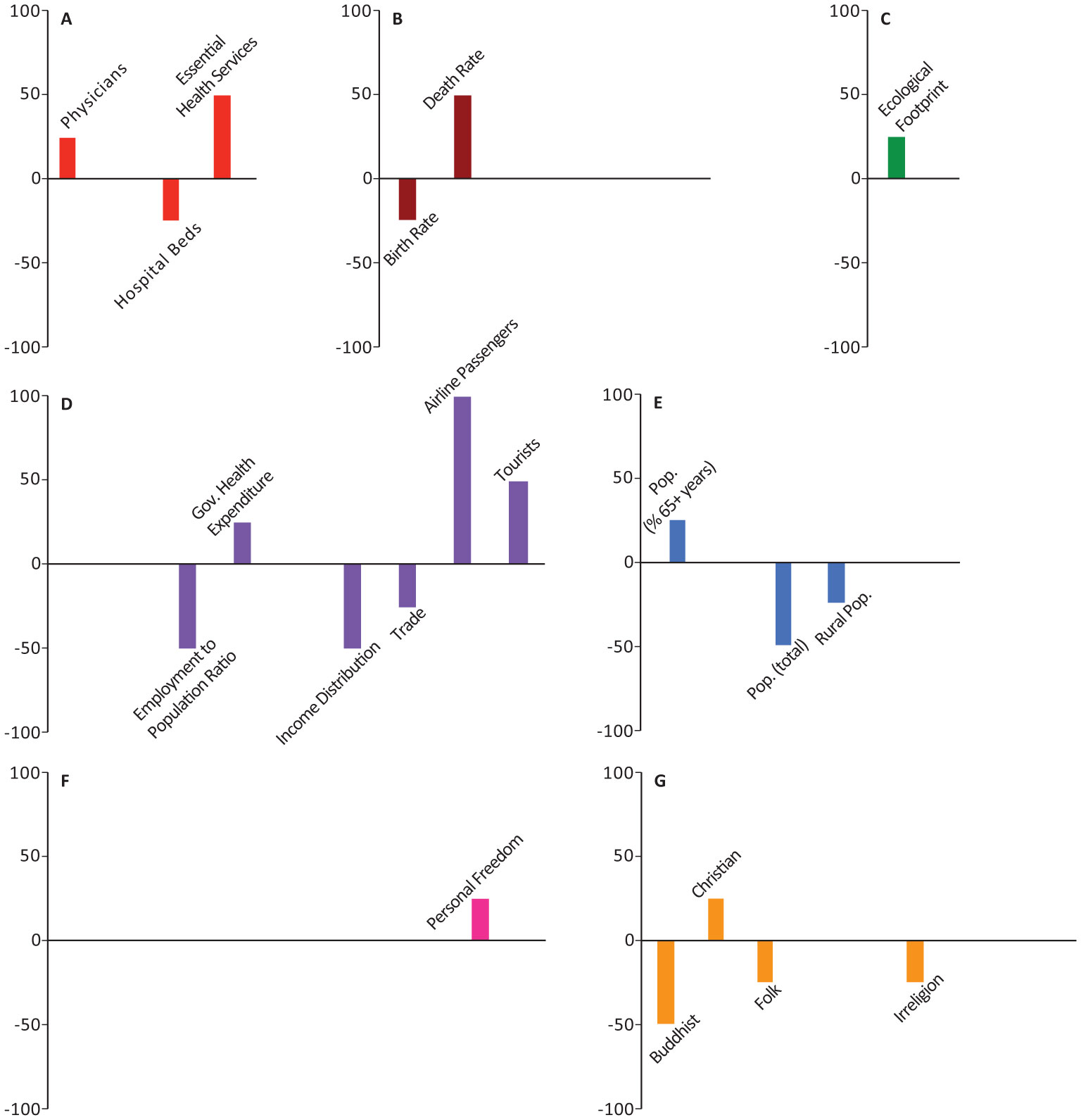
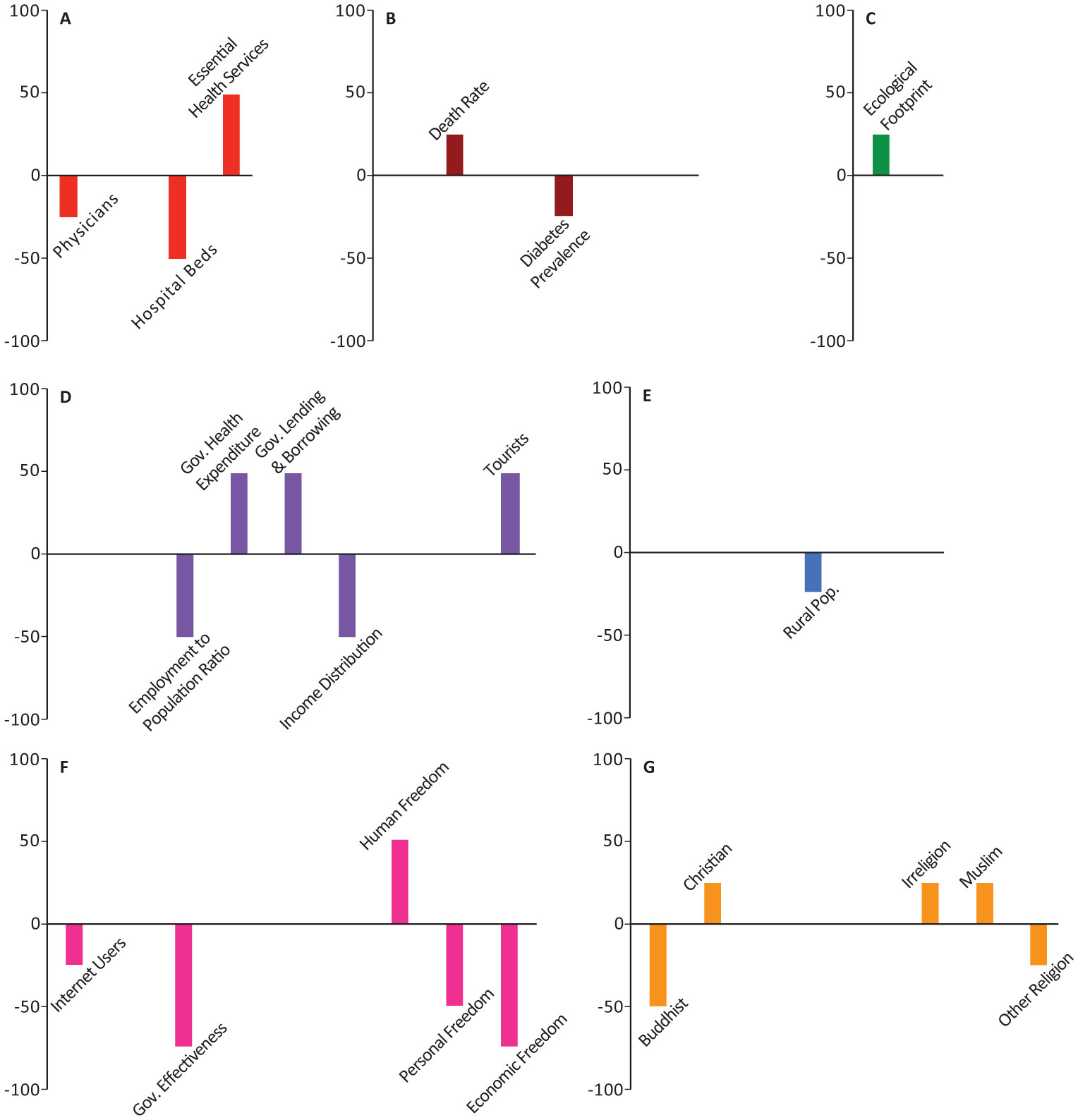
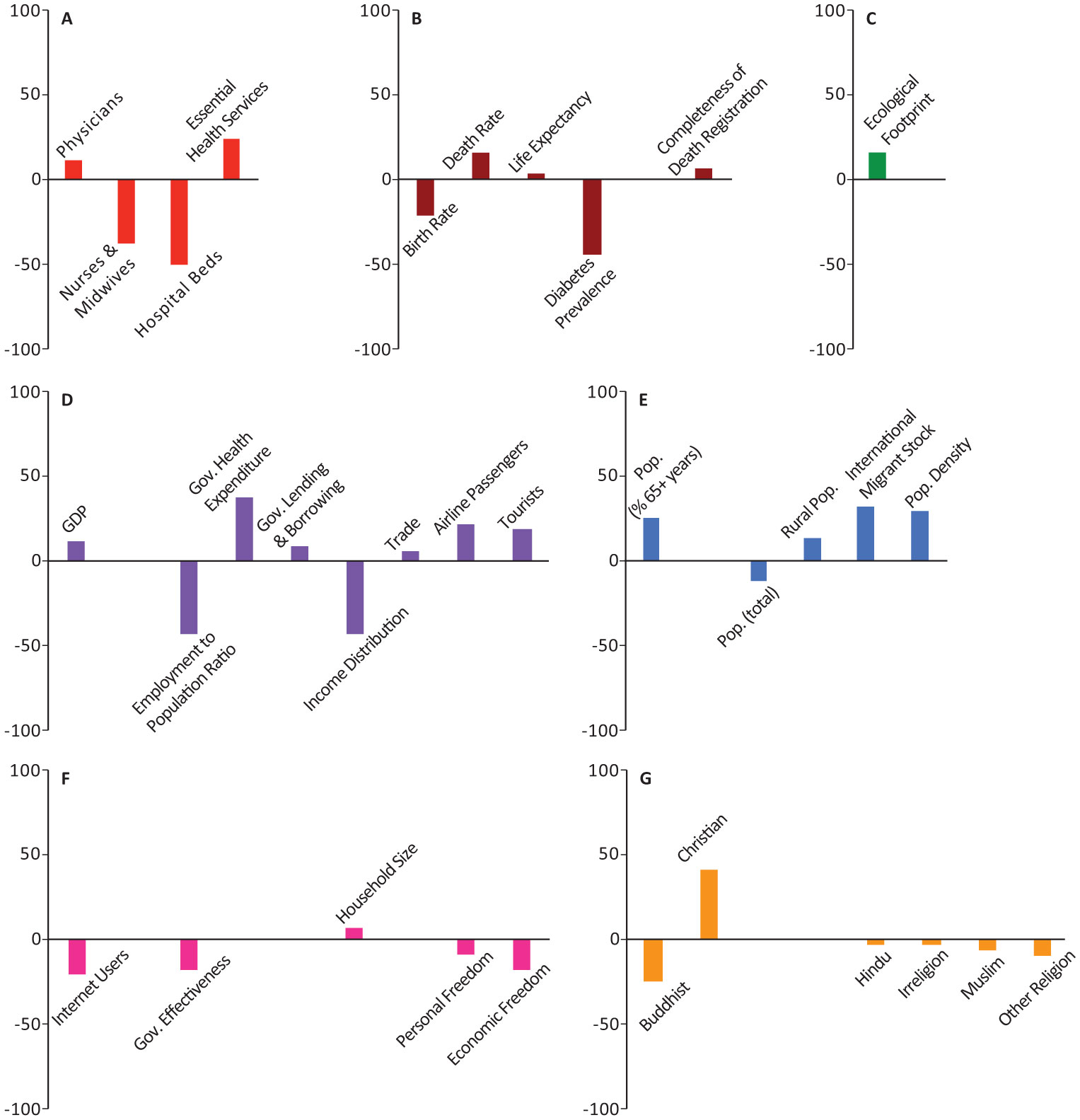
This study investigates the relationship between socio-economic determinants pre-dating the pandemic and the reported number of cases, deaths, and the ratio of deaths/cases in 199 countries/regions during the first months of the COVID-19 pandemic. The analysis is performed by means of machine learning methods. It involves a portfolio/ensemble of 32 interpretable models and considers the case in which the outcome variables (number of cases, deaths, and their ratio) are independent and the case in which their dependence is weighted based on geographical proximity. We build two measures of variable importance, the Absolute Importance Index (AII) and the Signed Importance Index (SII) whose roles are to identify the most contributing socio-economic factors to the variability of the COVID-19 pandemic. Our results suggest that, together with the established influence on cases and deaths of the level of mobility, the specific features of the health care system (smart/poor allocation of resources), the economy of a country (equity/non-equity), and the society (religious/not religious or community-based vs not) might contribute to the number of COVID-19 cases and deaths heterogeneously across countries.
Citation: Kathleen Lois Foster, Alessandro Maria Selvitella. On the relationship between COVID-19 reported fatalities early in the pandemic and national socio-economic status predating the pandemic[J]. AIMS Public Health, 2021, 8(3): 439-455. doi: 10.3934/publichealth.2021034
This study investigates the relationship between socio-economic determinants pre-dating the pandemic and the reported number of cases, deaths, and the ratio of deaths/cases in 199 countries/regions during the first months of the COVID-19 pandemic. The analysis is performed by means of machine learning methods. It involves a portfolio/ensemble of 32 interpretable models and considers the case in which the outcome variables (number of cases, deaths, and their ratio) are independent and the case in which their dependence is weighted based on geographical proximity. We build two measures of variable importance, the Absolute Importance Index (AII) and the Signed Importance Index (SII) whose roles are to identify the most contributing socio-economic factors to the variability of the COVID-19 pandemic. Our results suggest that, together with the established influence on cases and deaths of the level of mobility, the specific features of the health care system (smart/poor allocation of resources), the economy of a country (equity/non-equity), and the society (religious/not religious or community-based vs not) might contribute to the number of COVID-19 cases and deaths heterogeneously across countries.

| [1] | World Health Organization Rolling updates on coronavirus disease (COVID-19) (2020) .Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen. |
| [2] | Hilton J, Keeling MJ (2020) Estimation of country-level basic reproductive ratios for novel coronavirus (covid-19) using synthetic contact matrices. medRxiv 1-7. |
| [3] | Tuite A, Fisman DN, Greer AL (2020) Mathematical modeling of COVID-19 transmission and mitigation strategies in the population of Ontario, Canada. medRxiv 1-23. |
| [4] |
Giordano G, Blanchini F, Bruno R, et al. (2020) Modelling the COVID-19 epidemic and implementation of population-wide interventions in Italy. Nat Med 26: 855-860. doi: 10.1038/s41591-020-0883-7

|
| [5] | Stojkoski V, Utkovski Z, Jolakoski P, et al. (2020) The socio-economic determinants of the coronavirus disease (COVID-19) pandemic. medRxiv 1-22. |
| [6] |
Mikhael EM, Al-Jumaili AA (2020) Can developing countries alone face coronavirus? An Iraqi situation. Public Health Pract 1: 100004. doi: 10.1016/j.puhip.2020.100004
|
| [7] |
Di Marco M, Baker ML, Daszak P, et al. (2020) Opinion: Sustainable development must account for pandemic risk. Proc Nat Acad Sci 117: 3888-3892. doi: 10.1073/pnas.2001655117
|
| [8] | Ferguson NM, Laydon D, Nedjati-Gilani G, et al. (2020) Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College COVID-19 Response Team 1-20. |
| [9] |
Tian H, Liu Y, Li Y, et al. (2020) An investigation of transmission control measures during the first 50 days of the COVID-19 epidemic in China. Science 368: 638-642. doi: 10.1126/science.abb6105
|
| [10] |
Nicola M, Alsafi Z, Sohrabi C, et al. (2020) The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int J Surg 78: 185-193. doi: 10.1016/j.ijsu.2020.04.018
|
| [11] |
Ashraf BN (2020) Economic impact of government interventions during the COVID-19 pandemic: International evidence from financial markets. J Behav Exp Finance 27: 100371. doi: 10.1016/j.jbef.2020.100371
|
| [12] |
Poudel K, Subedi P (2020) Impact of COVID-19 pandemic on socioeconomic and mental health aspects in Nepal. Int J Soc Psychiatry 66: 748-755. doi: 10.1177/0020764020942247
|
| [13] | Our World In Data Coronavirus pandemic (COVID-19) (2020) .Available from: http://ourworldindata.org/. |
| [14] | World Bank Group World bank open data (2020) .Available from: https://data.worldbank.org/. |
| [15] | International Monetary Fund World economic outlook database (2020) .Available from: https://www.imf.org/en/data. |
| [16] | United Nations Household size and composition (2019) .Available from: https://population.un.org/Household/index.html#/countries/840. |
| [17] | Global Footprint Network National footprint and biocapacity accounts (2020) .Available from: http://data.footprintnetwork.org/#/. |
| [18] | Institute for Health Metrics and Evaluation State of Global Air (2020) .Available from: https://www.stateofglobalair.org/engage. |
| [19] | Vásquez I, Porčnik T (2019) The Human Freedom Index 2019: A Global Measurement of Personal, Civil, and Economic freedom Washington: Cato Institute, Fraser Institute, and the Friedrich Naumann Foundation for Freedom, Available from: https://www.cato.org/human-freedom-index-new. |
| [20] | Pew Research Center The global religious landscape (2012) .Available from: https://assets.pewresearch.org/wp-content/uploads/sites/11/2014/01/global-religion-full.pdf. |
| [21] |
Daskalakis C, Dikkala N, Panageas N (2019) Regression from sependent observations. STOC2019: Proceedings of the 51st Annual ACM SIGACT Symposium on the Theory of Computing 881-889. doi: 10.1145/3313276.3316362
|
| [22] | Van Buuren S, Groothuis-Oudshoorn K (2011) mice: Multivariate Imputation by Chained Equations in R. J Stat Soft 45: 1-67. |
| [23] |
Azur MJ, Stuart EA, Frangakis C, et al. (2011) Multiple imputation by chained equations: What is it and how does it work?.. Int J Methods Psychiatr Res 20: 40-49. doi: 10.1002/mpr.329
|
| [24] |
McCullagh P, Nedler JA (2019) Generalized Linear Models Boca Raton: Chapman and Hall/CRC. doi: 10.1201/9780203753736
|
| [25] | Selvitella AM, Foster KL (2020) Societal and economic factors associated with COVID-19 indicate that developing countries could suffer the most. Technium Soc Sci 10: 637-644. |
| [26] | Tibshirani R (1996) Regression Shrinkage and Selection via the lasso. J R Stat Soc B 58: 267-288. |
| [27] |
James G, Witten D, Tastie T, et al. (2013) Introduction to Statistical Learning New York: Springer. doi: 10.1007/978-1-4614-7138-7
|
| [28] | Jagodnik KM, Ray F, Giorgi FM, et al. (2020) Correcting under-reported COVID-19 case numbers: Estimating the true scale of the pandemic. medRxiv 1-6. |
| [29] |
Li R, Pei S, Chen B, et al. (2020) Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science 368: 489-493. doi: 10.1126/science.abb3221
|
| [30] |
Chowell G, Viboud C, Simonsen L, et al. (2016) Characterizing the reproduction number of epidemics with early sub-exponential growth dynamics. J R Soc Interface 13: 20160659. doi: 10.1098/rsif.2016.0659
|
| [31] | DeFranza D, Lindow M, Harrison K, et al. (2020) Religion and reactance to COVID-19 mitigation guidelines. Am Physchol 1-11. |
| [32] |
Shutta DP, Manorec CA, Pankavich S, et al. (2017) Estimating the reproductive number,total outbreak size, and reporting rates for zika epidemics in South and Central America. Epidemics 21: 63-79. doi: 10.1016/j.epidem.2017.06.005
|
 publichealth-08-03-034-s001.pdf publichealth-08-03-034-s001.pdf |
 |
Figures(6) / Tables(1)

Kathleen Lois Foster, Alessandro Maria Selvitella. On the relationship between COVID-19 reported fatalities early in the pandemic and national socio-economic status predating the pandemic[J]. AIMS Public Health, 2021, 8(3): 439-455. doi: 10.3934/publichealth.2021034







 DownLoad:
DownLoad: