Gut microbiomes play a role in developing and regulating autoimmune diseases such as multiple sclerosis (MS). We designed this systematic review to summarize the evidence of the effect of gut microbiota in developing pediatric-onset MS.
PubMed, Scopus, EMBASE, Web of Science, Google Scholar, references of the references and conference abstracts were comprehensively searched by two independent researchers. The search was done on January 1st, 2023. Data regarding the total number of patients, the name of the first author, publication year, country of origin, mean age, duration of the disease, body mass index (BMI), type of MS, Expanded Disability Status Scale (EDSS), age at disease onset and stool composition were extracted.
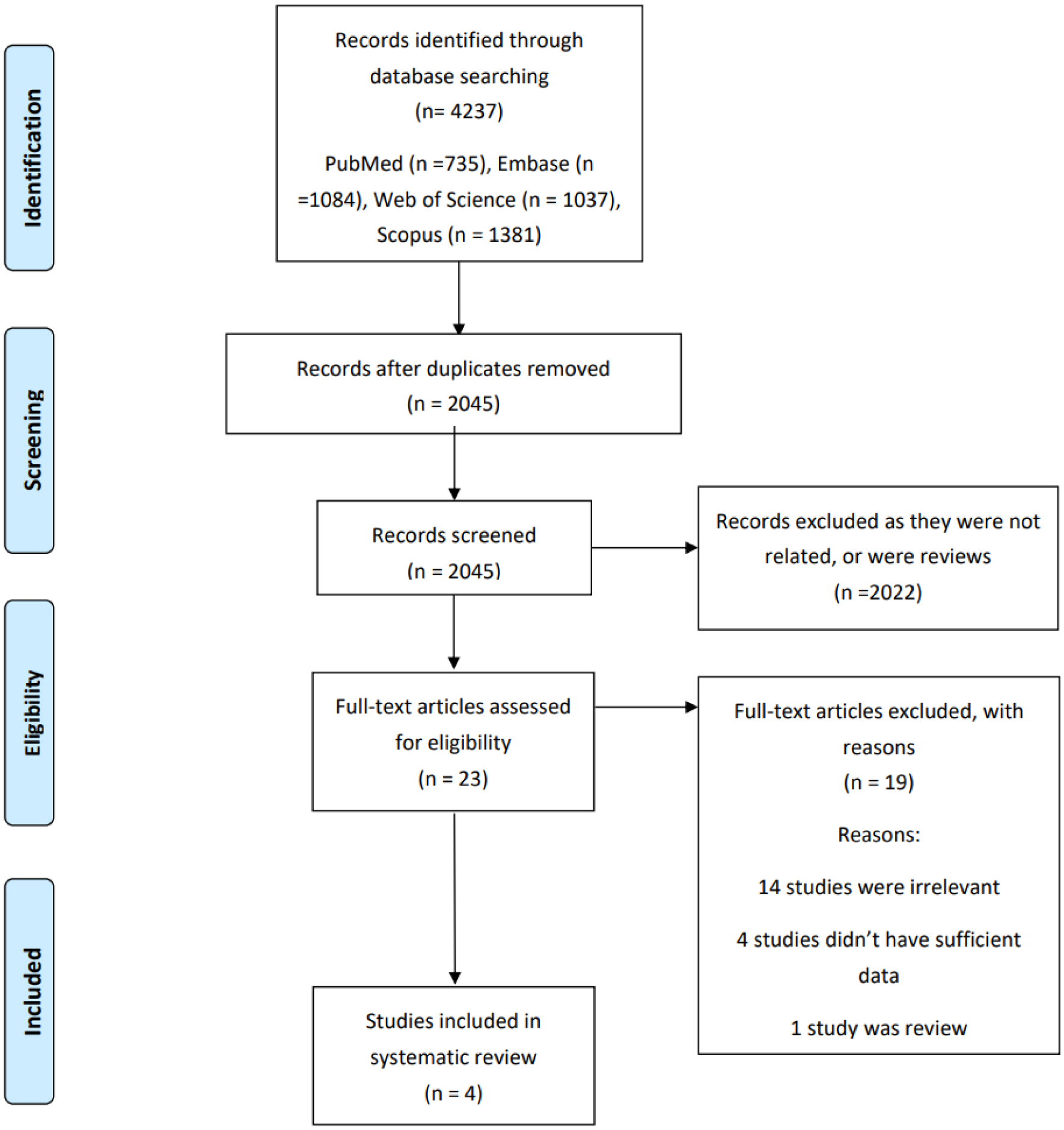
A literature search revealed 4237 published studies. After removing duplicates, we had 2045 records for evaluation. Twenty-three full texts were evaluated, and four case-control studies remained for systematic review. Three studies were conducted in the United States and one in the Netherlands. The number of participants in included studies ranged between 24 and 68. The mean age of patients at the time of study varied between 11.9 and 17.9 years, and the mean age at the onset of the disease ranged between 11.5 and 14.3 years. Most included patients were female. The results show that median richness (the number of unique taxa identified, which was provided by two studies) was higher in controls, and also Margalef index, which was reported by one study was higher in control group than the case group. The results of two studies also demonstrated that median evenness indexes (taxon distribution, Shannon, Simpson) were higher in control groups, as well as PD index (Faith's phylogenic diversity metric).
The result of this systematic review (including four studies) showed disruption of the microbiota-immune balance in pediatric-onset MS cases.
Citation: Sanaz Mehrabani, Mohsen Rastkar, Narges Ebrahimi, Mahsa Ghajarzadeh. Microbiomes and Pediatric onset multiple sclerosis (MS): A systematic review[J]. AIMS Neuroscience, 2023, 10(4): 423-432. doi: 10.3934/Neuroscience.2023031
Gut microbiomes play a role in developing and regulating autoimmune diseases such as multiple sclerosis (MS). We designed this systematic review to summarize the evidence of the effect of gut microbiota in developing pediatric-onset MS.
PubMed, Scopus, EMBASE, Web of Science, Google Scholar, references of the references and conference abstracts were comprehensively searched by two independent researchers. The search was done on January 1st, 2023. Data regarding the total number of patients, the name of the first author, publication year, country of origin, mean age, duration of the disease, body mass index (BMI), type of MS, Expanded Disability Status Scale (EDSS), age at disease onset and stool composition were extracted.
A literature search revealed 4237 published studies. After removing duplicates, we had 2045 records for evaluation. Twenty-three full texts were evaluated, and four case-control studies remained for systematic review. Three studies were conducted in the United States and one in the Netherlands. The number of participants in included studies ranged between 24 and 68. The mean age of patients at the time of study varied between 11.9 and 17.9 years, and the mean age at the onset of the disease ranged between 11.5 and 14.3 years. Most included patients were female. The results show that median richness (the number of unique taxa identified, which was provided by two studies) was higher in controls, and also Margalef index, which was reported by one study was higher in control group than the case group. The results of two studies also demonstrated that median evenness indexes (taxon distribution, Shannon, Simpson) were higher in control groups, as well as PD index (Faith's phylogenic diversity metric).
The result of this systematic review (including four studies) showed disruption of the microbiota-immune balance in pediatric-onset MS cases.

| [1] | Ghajarzadeh M, Mahsa O, Sauraian MA, et al. (2014) Emotional intelligence (EI) of patients with multiple sclerosis (MS). Iran J Public Health 43: 1550. |
| [2] | Eskandari G, Ghajarzadeh M, Yekaninejad MS, et al. (2015) Comparison of serum vitamin D level in multiple sclerosis patients, their siblings, and healthy controls. Iran J Neurol 14: 81. |
| [3] |
Gensollen T, Iyer SS, Kasper DL, et al. (2016) How colonization by microbiota in early life shapes the immune system. Science 352: 539-44. https://doi.org/10.1126/science.aad9378 
|
| [4] |
Berer K, Mues M, Koutrolos M, et al. (2011) Commensal microbiota and myelin autoantigen cooperate to trigger autoimmune demyelination. Nature 479: 538-41. https://doi.org/10.1038/nature10554
|
| [5] |
Lee YK, Menezes JS, Umesaki Y, et al. (2011) Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. P Natl A Sci 108: 4615-22. https://doi.org/10.1073/pnas.1000082107
|
| [6] |
Maynard CL, Elson CO, Hatton RD, et al. (2012) Reciprocal interactions of the intestinal microbiota and immune system. Nature 489: 231-41. https://doi.org/10.1038/nature11551
|
| [7] |
Sampson TR, Mazmanian SK (2015) Control of brain development, function, and behavior by the microbiome. Cell Host Microbe 17: 565-76. https://doi.org/10.1016/j.chom.2015.04.011
|
| [8] |
Mirza A, Forbes JD, Zhu F, et al. (2020) The multiple sclerosis gut microbiota: A systematic review. Mult Scler Relat Dis 37: 101427. https://doi.org/10.1016/j.msard.2019.101427
|
| [9] |
Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 88: 105906. https://doi.org/10.1016/j.ijsu.2021.105906
|
| [10] | Peterson J, Welch V, Losos M, et al. (2011) The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute 1-12. |
| [11] |
Tremlett H, Fadrosh DW, Faruqi AA, et al. (2016) Associations between the gut microbiota and host immune markers in pediatric multiple sclerosis and controls. BMC Neurol 16: 1-9. https://doi.org/10.1186/s12883-016-0703-3
|
| [12] |
Bruijstens AL, Molenaar S, Wong YYM, et al. (2022) Gut microbiota analysis in pediatric-onset multiple sclerosis compared to pediatric monophasic demyelinating syndromes and pediatric controls. Eur J Neurol 30: 3507-3515. https://doi.org/10.1111/ene.15594
|
| [13] |
Tremlett H, Fadrosh DW, Faruqi AA, et al. (2016) Gut microbiota in early pediatric multiple sclerosis: a case-control study. Eur J Neurol 23: 1308-21. https://doi.org/10.1111/ene.13026
|
| [14] |
Tremlett H, Zhu F, Arnold D, et al. (2021) The gut microbiota in pediatric multiple sclerosis and demyelinating syndromes. Ann Clin Transl Neur 8: 2252-69. https://doi.org/10.1002/acn3.51476
|
| [15] |
Chen J, Chia N, Kalari KR, et al. (2016) Multiple sclerosis patients have a distinct gut microbiota compared to healthy controls. Sci Rep 6: 1-10. https://doi.org/10.1038/srep28484
|
| [16] |
Cekanaviciute E, Yoo BB, Runia TF, et al. (2017) Gut bacteria from multiple sclerosis patients modulate human T cells and exacerbate symptoms in mouse models. P Natl A Sci 114: 10713-8. https://doi.org/10.1073/pnas.1711235114
|
| [17] |
Berer K, Gerdes LA, Cekanaviciute E, et al. (2017) Gut microbiota from multiple sclerosis patients enables spontaneous autoimmune encephalomyelitis in mice. P Natl A Sci 114: 10719-24. https://doi.org/10.1073/pnas.1711233114
|
| [18] |
Berer K, Krishnamoorthy G (2014) Microbial view of central nervous system autoimmunity. FEBS Lett 588: 4207-13. https://doi.org/10.1016/j.febslet.2014.04.007
|
Figures(1) / Tables(1)

Sanaz Mehrabani, Mohsen Rastkar, Narges Ebrahimi, Mahsa Ghajarzadeh. Microbiomes and Pediatric onset multiple sclerosis (MS): A systematic review[J]. AIMS Neuroscience, 2023, 10(4): 423-432. doi: 10.3934/Neuroscience.2023031







 DownLoad:
DownLoad: