Citation: Sudip Bhattacharya, Amarjeet Singh, Roy Rillera Marzo. Delivering emoji/icon-based universal health education messages through smartphones[J]. AIMS Public Health, 2019, 6(3): 242-247. doi: 10.3934/publichealth.2019.3.242

| [1] | Bhattacharya S, Singh A (2016) Opportunity of Health Sector in IT Applications-A Case Study from Tribal Area of West Bengal. Int J HealthCare Edu Med 3: 1. |
| [2] |
Bhattacharya S, Kumar A, Kaushal V, et al. (2018) Applications of m-Health and e-Health in Public Health Sector: The Challenges and Opportunities. Int J Med Public Health 8: 56–57. doi: 10.5530/ijmedph.2018.2.12

|
| [3] | World Health Organization (2015) WHO compendium of innovative health technologies for low-resource settings, 2011–2014: assistive devices, eHealth solutions, medical devices, other technologies, technologies for outbreaks, Geneva, Switzerland: WHO Press, 142. |
| [4] |
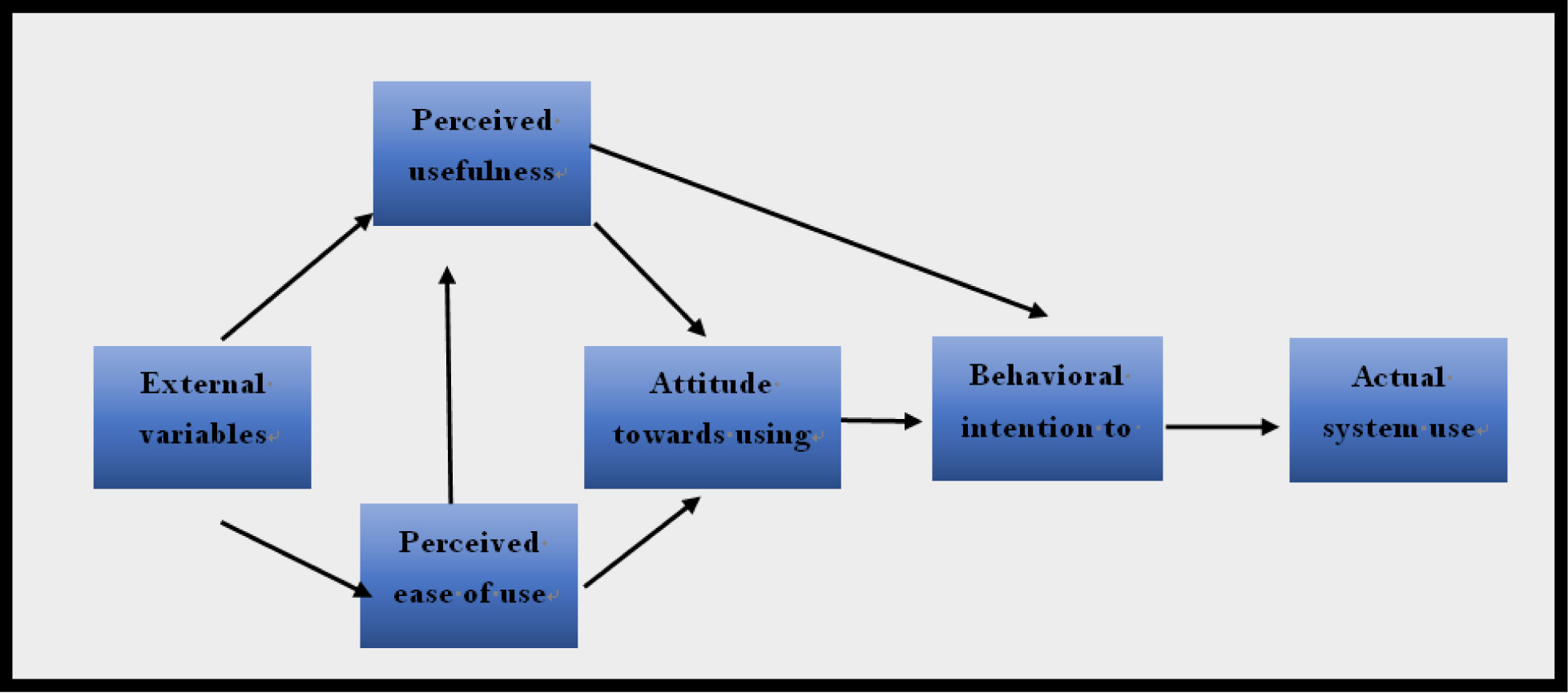
Davis FD (1989) Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Quarterly 13: 319. doi: 10.2307/249008
|
| [5] |
Cresswell KM, Bates DW, Sheikh A (2013) Ten key considerations for the successful implementation and adoption of large-scale health information technology. J Am Med Inf Assoc 20: e9–13. doi: 10.1136/amiajnl-2013-001684
|
| [6] | Harari YN (2018) 21 Lessons for the 21st Century, Random House, London: Jonathan Cape. |
| [7] | Telecom Industry in India. (2019) Available from: https://www.ibef.org/industry/telecommunications.aspx |
| [8] |
Moriyama M, Harnisch DL, Matsubara S (1994) The development of graphic symbols for medical symptoms to facilitate communication between health care providers and receivers. Tohoku J Exp Med 174: 387–398. doi: 10.1620/tjem.174.387
|
| [9] | Kaur S, Nagi M, Gupta SK, et al. (2018) How to take care of the patients at home after Neurosurgery-A Guide Book, Chandigarh, Mohindra publishing house. |
| [10] | About the Linguistic Survey of India (2019). Available from: https://dsal.uchicago.edu/books/lsi/about-lsi.html. |
| [11] | Bhattacharya S, Bashar MA, Singh A (2017) So near, yet so far: access to safe abortion services remains elusive for poor women in India. BMJ Case Rep 13: bcr-2017-220980. |
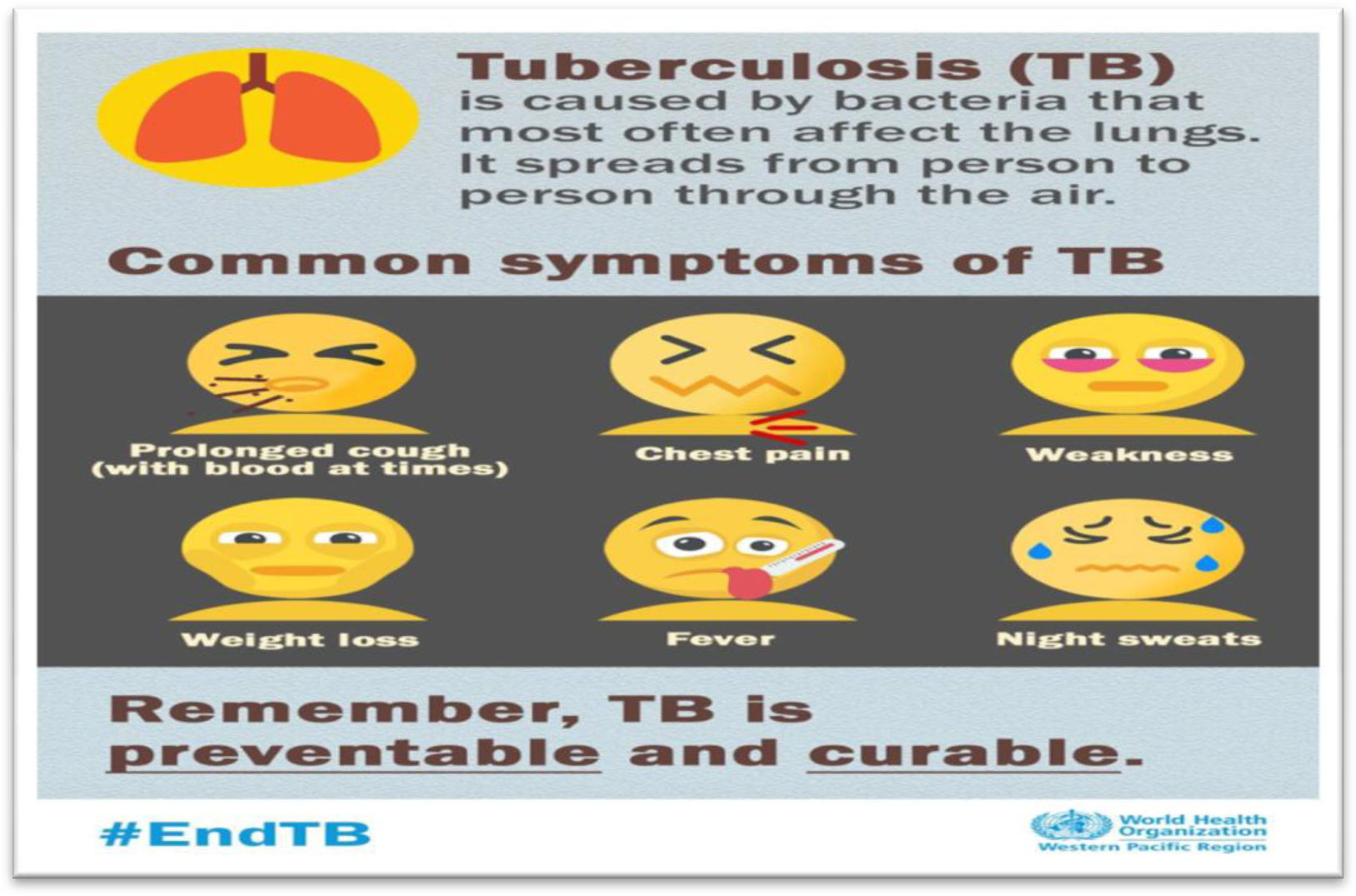
| [12] | Bhattacharya S, Singh A (2017) Why tuberculosis control programmes fail? Role of microlevel and macrolevel factors: an analysis from India. BMJ Case Rep 21: bcr-2017-219606. |
| [13] | Bhattacharya S, Singh A (2018) Beliefs of a traditional rural Indian family towards naturalistic and faith healing for treating epilepsy: a case study. BMJ Case Rep 17: bcr-2018-225405. |
| [14] | Bhattacharya S, Singh A (2016) How effective is the Menstrual Hygiene Scheme? An evaluation study from North India. Int J Community Med Public Health 3: 2584–2586. |
| [15] | Agarwal SK, Srivastava RK, Gupta S, et al. (2012) Evolution of the Transplantation of Human Organ Act and law in India. Transplantat 94: 110–113. |
| [16] |
Kumar R, Bhattacharya S, Sharma N, et al. (2019) Cultural competence in family practice and primary care setting. J Family Med Primary Care 8: 1. doi: 10.4103/jfmpc.jfmpc_393_18
|
| [17] |
Bhattacharya S, Sharma N, Singh A (2019) Designing culturally acceptable screening for breast cancer through artificial intelligence-two case studies. J Family Med Primary Care 8: 760. doi: 10.4103/jfmpc.jfmpc_391_18
|

Figures(3)

Sudip Bhattacharya, Amarjeet Singh, Roy Rillera Marzo. Delivering emoji/icon-based universal health education messages through smartphones[J]. AIMS Public Health, 2019, 6(3): 242-247. doi: 10.3934/publichealth.2019.3.242







 DownLoad:
DownLoad: