Citation: Elham Hatef, Zachary Predmore, Elyse C. Lasser, Hadi Kharrazi, Karin Nelson, Idamay Curtis, Stephan Fihn, Jonathan P. Weiner. Integrating social and behavioral determinants of health into patient care and population health at Veterans Health Administration: a conceptual framework and an assessment of available individual and population level data sources and evidence-based measurements[J]. AIMS Public Health, 2019, 6(3): 209-224. doi: 10.3934/publichealth.2019.3.209

| [1] |
Bazemore AW, Cottrell EK, Gold R, et al. (2016) Community vital signs: Incorporating geocoded social determinants into electronic records to promote patient and population health. J Am Med Inform Assoc 23: 407–412. doi: 10.1093/jamia/ocv088

|
| [2] | McGinnis JM, Williams-Russo P, Knickman JR (2002) The case for more active policy attention to health promotion. Health Aff (Millwood) 21: 78–93. |
| [3] | Adler NE, Cutler DM, Fielding JE, et al. (2016) Addressing social determinants of health and health disparities. discussion paper, vital directions for health and health care series. Available from: https://nam.edu/wp-content/uploads/2016/09/Addressing-Social-Determinants-of-Health-and-Health-Disparities.pdf. |
| [4] | Moy E, Chang E, Barrett M (2013) Centers for Disease Control and Prevention, (CDC): Potentially preventable hospitalizations-United States, 2001–2009. MMWR Suppl 62: 139–143. |
| [5] | Value-based programs (2018) Available from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/Value-Based-Programs.html. |
| [6] | Hong CS, Siegel AL, Ferris TG (2014) Caring for high-need, high-cost patients: What makes for a successful care management program?. Issue Brief (Commonw Fund) 19: 1–19. |
| [7] | Wenger M (2012) Place matters: Ensuring opportunities for good health for all-A summary of place matters' community health equity reports. Available from: http://jointcenter.org/sites/default/files/Place%20Matters%20Community%20Reports%20Summary.pdf. |
| [8] |
Katz A, Chateau D, Enns JE, et al. (2018) Association of the social determinants of health with quality of primary care. Ann Fam Med 16: 217–224. doi: 10.1370/afm.2236
|
| [9] |
Sandberg SF, Erikson C, Owen R, et al. (2014) Hennepin health: A safety-net accountable care organization for the expanded Medicaid population. Health Aff (Millwood) 33: 1975–1984. doi: 10.1377/hlthaff.2014.0648
|
| [10] |
Taylor LA, Tan AX, Coyle CE, et al. (2016) Leveraging the social determinants of health: What works? PLoS One 11: e0160217. doi: 10.1371/journal.pone.0160217
|
| [11] |
DeVoe JE, Bazemore AW, Cottrell EK (2016) Perspectives in primary care: A conceptual framework and path for integrating social determinants of health into primary care practice. Ann Fam Med 14: 104–108. doi: 10.1370/afm.1903
|
| [12] |
Tipirneni R, Vickery KD, Ehlinger EP (2015) Accountable communities for health: Moving from providing accountable care to creating health. Ann Fam Med 13: 367–369. doi: 10.1370/afm.1813
|
| [13] | Predmore Z, Hatef E, Weiner JP (2019) Integrating Social and Behavioral Determinants of Health into Population Health Analytics: A Conceptual Framework and Suggested Road Map. Popul Health Manag. |
| [14] |
Nelson K, Schwartz G, Hernandez S, et al. (2017) The association between neighborhood environment and mortality: Results from a national study of veterans. J Gen Intern Med 32: 416–422. doi: 10.1007/s11606-016-3905-x
|
| [15] |
Lushniak BD, Alley DE, Ulin B, et al. (2015) The national prevention strategy: Leveraging multiple sectors to improve population health. Am J Public Health 105: 229–231. doi: 10.2105/AJPH.2014.302257
|
| [16] |
Hatef E, Searle KM, Predmore Z, et al. (2019) The Impact of Social Determinants of Health on Hospitalization in the Veterans Health Administration. Am J Prev Med 56: 811–818. doi: 10.1016/j.amepre.2018.12.012
|
| [17] | Rosland AM, Nelson K, Sun H, et al. (2013) The patient-centered medical home in the veterans' health administration. Am J Manag Care 19: e263–e272. |
| [18] | Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records, Board on Population Health and Public Health Practice, Institute of Medicine. (2014) Capturing social and behavioral domains and measures in electronic health records: Phase 2, Washington, D.C: National Academies Press. Available from: https://www.nap.edu/resource/18951/EHRreportbrief.pdf. |
| [19] |
Juarez PD, Matthews-Juarez P, Hood DB, et al. (2014) The public health exposome: a population-based, exposure science approach to health disparities research. Int J Environ Res Public Health 11: 12866–12895. doi: 10.3390/ijerph111212866
|
| [20] |
Remington PL, Catlin BB, Gennuso KP (2015) The county health rankings: Rationale and methods. Popul Health Metr 13: 11. doi: 10.1186/s12963-015-0044-2
|
| [21] |
Rosen AK, Reid R, Broemeling AM, et al. (2003) Applying a risk adjustment framework to primary care: can we improve on existing measures? Ann Fam Med 1: 44–51. doi: 10.1370/afm.6
|
| [22] | Box T, Fihn S (2017) The patient care assessment system (PCAS) 2.0 and care assessment needs score 2.0: Two tools for PACT teams. U.S. Department of Veterans Affairs. Health Services Research and Development Web site. Available from: https://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/video_archive.cfm?SessionID=1088. |
| [23] |
Arthur KC, Lucenko BA, Sharkova IV, et al. (2018) Using state administrative data to identify social complexity risk factors for children. Ann Fam Med 16: 62–69. doi: 10.1370/afm.2134
|
| [24] | The United States Census Bureau. American community survey (ACS). Available from: https://www.census.gov/programs-surveys/acs/. |
| [25] |
Kansagara D, Englander H, Salanitro A, et al. (2011) Risk prediction models for hospital readmission: A systematic review. JAMA 306: 1688–1698. doi: 10.1001/jama.2011.1515
|
| [26] |
Nagasako EM, Reidhead M, Waterman B, et al. (2014) Adding socioeconomic data to hospital readmissions calculations may produce more useful results. Health Aff (Millwood) 33: 786–791. doi: 10.1377/hlthaff.2013.1148
|
| [27] | The Center for Health Care Strategies (2016) Measuring social determinants of health among low-income populations: Early insights from state initiatives. Available from: http://www.chcs.org/resource/measuring-social-determinants-health-among-low-income-populations-early-insights-state-initiatives/. |
| [28] |
Buck DS, Brown CA, Mortensen K, et al. (2012) Comparing homeless and domiciled patients' utilization of the Harris county, Texas public hospital system. J Health Care Poor Underserved 23: 1660–1670. doi: 10.1353/hpu.2012.0171
|
| [29] |
Brown RT, Miao Y, Mitchell SL, et al. (2015) Health outcomes of obtaining housing among older homeless adults. Am J Public Health 105: 1482–1488. doi: 10.2105/AJPH.2014.302539
|
| [30] |
Juhn YJ, Beebe TJ, Finnie DM, et al. (2011) Development and initial testing of a new socioeconomic status measure based on housing data. J Urban Health 88: 933–944. doi: 10.1007/s11524-011-9572-7
|
| [31] |
Burgard SA, Seefeldt KS, Zelner S (2012) Housing instability and health: Findings from the Michigan recession and recovery study. Soc Sci Med 75: 2215–2224. doi: 10.1016/j.socscimed.2012.08.020
|
| [32] |
Rohe WM, Stewart LS (1996) Homeownership and neighborhood stability. Hous Policy Debate 7: 37–81. doi: 10.1080/10511482.1996.9521213
|
| [33] |
Navathe AS, Zhong F, Lei VJ, et al. (2018) Hospital readmission and social risk factors identified from physician notes. Health Serv Res 53: 1110–1136. doi: 10.1111/1475-6773.12670
|
| [34] | Executive Office of Health and Human Services (2016) Mass health risk adjustment model social determinants of health. Available from: http://www.mass.gov/eohhs/docs/eohhs/healthcare-reform/masshealth-innovations/1610-risk-adjustment-open-public-meeting.pdf. |
| [35] | Ash AS, Mick E (2016) UMass risk adjustment project for mass health payment and care delivery reform: Describing the 2017 payment model. Available from: http://www.mass.gov/eohhs/docs/eohhs/healthcare-reform/masshealth-innovations/1610-umass-modeling-sdh-summary-report.pdf. |
| [36] | Virginia Department of Health (2012) Virginia health opportunity index (HOI). Available from: http://www.vdh.virginia.gov/health-equity/virginia-health-opportunity-index-hoi/. |
| [37] | Glazier RH, Creatore MI, Weyman JT, et al. (2014) Density, destinations or both? A comparison of measures of walkability in relation to transportation behaviors, obesity and diabetes in Toronto, Canada. PloS One 9: e85295. |
| [38] |
Leonardi C, Simonsen NR, Yu Q, et al. (2017) Street connectivity and obesity risk: Evidence from electronic health records. Am J Prev Med 52: S40–S47. doi: 10.1016/j.amepre.2016.09.029
|
| [39] |
Rohrer J, Pierce JR, Denison A (2004) Walkability and self-rated health in primary care patients. BMC Fam Pract 5: 29. doi: 10.1186/1471-2296-5-29
|
| [40] |
Zhu X, Lee C (2008) Walkability and safety around elementary schools economic and ethnic disparities. Am J Prev Med 34: 282–290. doi: 10.1016/j.amepre.2008.01.024
|
| [41] |
Carroll-Scott A, Gilstad-Hayden K, Rosenthal L, et al. (2013) Disentangling neighborhood contextual associations with child body mass index, diet, and physical activity: The role of built, socioeconomic, and social environments. Soc Sci Med 95: 106–144. doi: 10.1016/j.socscimed.2013.04.003
|
| [42] |
Morland K, Diez Roux AV, Wing S (2006) Supermarkets, other food stores, and obesity: The atherosclerosis risk in communities study. Am J Prev Med 30: 333–339. doi: 10.1016/j.amepre.2005.11.003
|
| [43] |
Ghosh-Dastidar B, Cohen D, Hunter G, et al. (2014) Distance to store, food prices, and obesity in urban food deserts. Am J Prev Med 47: 587–595. doi: 10.1016/j.amepre.2014.07.005
|
| [44] |
Fleischhacker SE, Evenson KR, Rodriguez DA, et al. (2011) A systematic review of fast food access studies. Obes Rev 12: e460–e471. doi: 10.1111/j.1467-789X.2010.00715.x
|
| [45] |
Kushel M, Gupta R, Gee L, et al. (2006) Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med 21: 71–77. doi: 10.1111/j.1525-1497.2005.00278.x
|
| [46] |
Calvillo-King L, Arnold D, Eubank KJ, et al. (2013) Impact of social factors on risk of readmission or mortality in pneumonia and heart failure: Systematic review. J Gen Intern Med 28: 269–282. doi: 10.1007/s11606-012-2235-x
|
| [47] | Krishnamurthi N, Francis J, Fihn SD, et al. (2018) Leading causes of cardiovascular hospitalization in 8.45 million US veterans. PLoS One 13: e0193996. |
| [48] |
Hu J, Gonsahn MD, Nerenz DR (2014) Socioeconomic status and readmissions: Evidence from an urban teaching hospital. Health Aff (Millwood) 33: 778–785. doi: 10.1377/hlthaff.2013.0816
|
| [49] |
Bhavsar NA, Gao A, Phelan M, et al. (2018) Value of neighborhood socioeconomic status in predicting risk of outcomes in studies that use electronic health record data. JAMA Network Open 1: e182716-e182716. doi: 10.1001/jamanetworkopen.2018.2716
|
| [50] | Liu SY, Pearlman DN (2009) Hospital readmissions for childhood asthma: The role of individual and neighborhood factors. Public Health Rep 124: 65–78. |
| [51] |
Beck AF, Huang B, Chundur R, et al. (2014) Housing code violation density associated with emergency department and hospital use by children with asthma. Health Affairs 33: 1993–2002. doi: 10.1377/hlthaff.2014.0496
|
| [52] |
Gronlund C, Zanobetti A, Wellenius G, et al. (2016) Vulnerability to renal, heat and respiratory hospitalizations during extreme heat among U.S. elderly. Clim Change 136: 631–645. doi: 10.1007/s10584-016-1638-9
|
| [53] |
Xu S, Fortney JC, Dong F (2009) Community-level correlates of hospitalizations for persons with schizophrenia. Psychiatr Serv 60: 772–778. doi: 10.1176/ps.2009.60.6.772
|
| [54] |
Harkness J, Newman SJ, Salkever D (2004) The Cost‐Effectiveness of independent housing for the chronically mentally ill: Do housing and neighborhood features matter? Health Serv Res 39: 1341–1360. doi: 10.1111/j.1475-6773.2004.00293.x
|
| [55] | Hatef E, Lasser EC, Kharrazi HHK, et al. (2017) A population health measurement framework: Evidence-based metrics for assessing community-level population health in the global budget context. Popul Health Manag 21: 261–270. |
| [56] |
Kharrazi H, Anzaldi LJ, Hernandez L, et al. (2018) The value of unstructured electronic health record data in geriatric syndrome case identification. J Am Geriatr Soc 66: 1499–1507. doi: 10.1111/jgs.15411
|
| [57] | Wang L, Ruan X, Yang P, et al. (2016) Comparison of three information sources for smoking information in electronic health records. Cancer Inform 15: 237–242. |
| [58] |
Torres J, Lawlor J, Colvin J, et al. (2017) ICD social codes: An underutilized resource for tracking social needs. Med Care 55: 810–816. doi: 10.1097/MLR.0000000000000764
|
| [59] |
Oreskovic NM, Maniates J, Weilburg J, et al. (2017) Optimizing the use of electronic health records to identify high-risk psychosocial determinants of health. JMIR Med Inform 5: e25. doi: 10.2196/medinform.8240
|
| [60] |
Cantor MN, Thorpe L (2018) Integrating data on social determinants of health into electronic health records. Health Affairs 37: 585–590. doi: 10.1377/hlthaff.2017.1252
|
| [61] | US Department of Health and Human Services (2016) Edition Health Information Technology (Health IT) Certification Criteria, 2015 Edition Base Electronic Health Record (EHR) Definition, and ONC Health IT Certification Program Modifications. |
| [62] | Centers for Medicare and Medicaid Services (2010) Meaningful Use Stage 1 Requirements Overview. Available from: https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/mu_stage1_reqoverview.pdf. |
| [63] | Centers for Medicare and Medicaid Services. Updated 2018 CMS QRDA III Implementation Guide for Eligible Clinicians and Eligible Professionals. Available from: https://ecqi.healthit.gov/ecqms/ecqm-news/now-available-updated-2018-cms-qrda-iii-implementation-guide-eligible-clinicians-0. |
| [64] |
Woolf SH, Dekker MM, Byrne FR, et al. (2011) Citizen-centered health promotion: building collaborations to facilitate healthy living. Am J Prev Med 40: S38–S47. doi: 10.1016/j.amepre.2010.09.025
|
| [65] |
Lindau ST, Makelarski J, Abramsohn E, et al. (2016) CommunityRx: A Population Health Improvement Innovation That Connects Clinics To Communities. Health Aff (Millwood) 35: 2020–2029. doi: 10.1377/hlthaff.2016.0694
|
| [66] | Hong CS, Siegel AL, Ferris TG (2014) Caring for high-need, high-cost patients: What makes for a successful care management program? Issue Brief (Commonw Fund) 19: 1–19. |
 publichealth-06-03-209-s001.pdf publichealth-06-03-209-s001.pdf |
 |
Figures(1) / Tables(2)

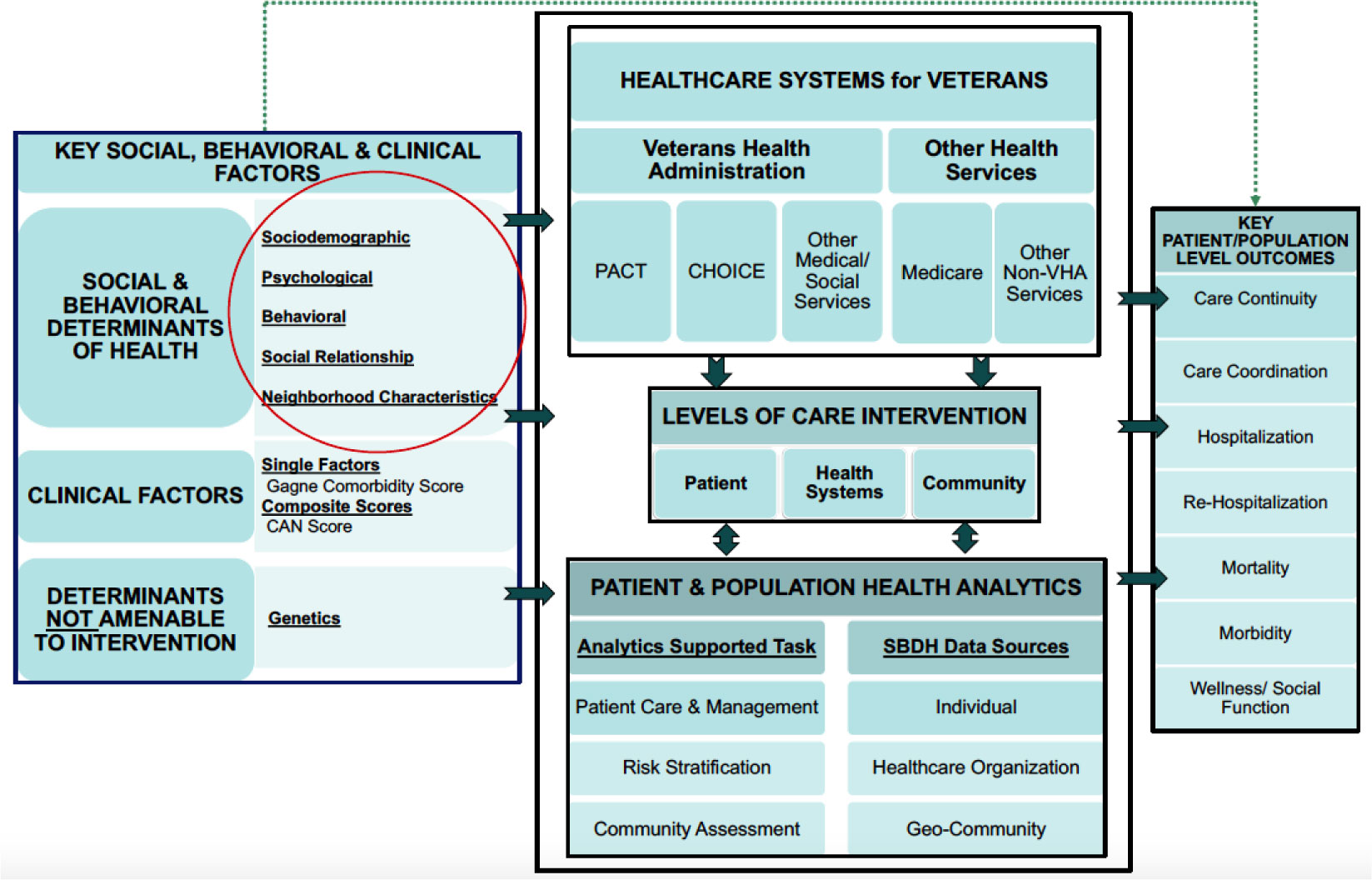
Elham Hatef, Zachary Predmore, Elyse C. Lasser, Hadi Kharrazi, Karin Nelson, Idamay Curtis, Stephan Fihn, Jonathan P. Weiner. Integrating social and behavioral determinants of health into patient care and population health at Veterans Health Administration: a conceptual framework and an assessment of available individual and population level data sources and evidence-based measurements[J]. AIMS Public Health, 2019, 6(3): 209-224. doi: 10.3934/publichealth.2019.3.209







 DownLoad:
DownLoad: