Citation: Joachim P Sturmberg, Geoff M McDonnell. How Modelling could Contribute to Reforming Primary Care—Tweaking “the Ecology of Medical Care” in Australia[J]. AIMS Medical Science, 2016, 3(3): 298-311. doi: 10.3934/medsci.2016.3.298

| [1] | Harrison D (2014) Health minster Peter Duton says Medicare spending unsustainable. Sydney Morning Herald. Sect. http://www.smh.com.au/federal-politics/political-news/medicare-unsustainable-without-overhaul-says-peterdutton-20140103-309ss.html. |
| [2] | Owens J (2014) Price signal needed to make Medicae sustaibable, says Dutton. The Australian. Sect. http://www.theaustralian.com.au/national-affairs/price-signal-needed-to-make-medicare-sustainable-says-dutton/story-fn59niix-1227136552889. |
| [3] | Owens J (2015) Government abandons plan to cut Medicare rebate for short GP visits. The Australian. Sect. http://www.theaustralian.com.au/national-affairs/health/government-abandons-plan-to-cut-medicare-rebatefor-short-gp-visits/story-fn59nokw-1227185738483. |
| [4] | Horn RE, Weber RP (2007) New Tools For Resolving Wicked Problems: Mess Mapping and Resolution Mapping Processes. San Francisco: Strategy Kinetics L.L.C.. |
| [5] |
Rittel HWJ, Webber MM (1973) Dilemmas in a General Theory of Planning Policy Sciences. Pol Sci 4: 155-169. doi: 10.1007/BF01405730

|
| [6] |
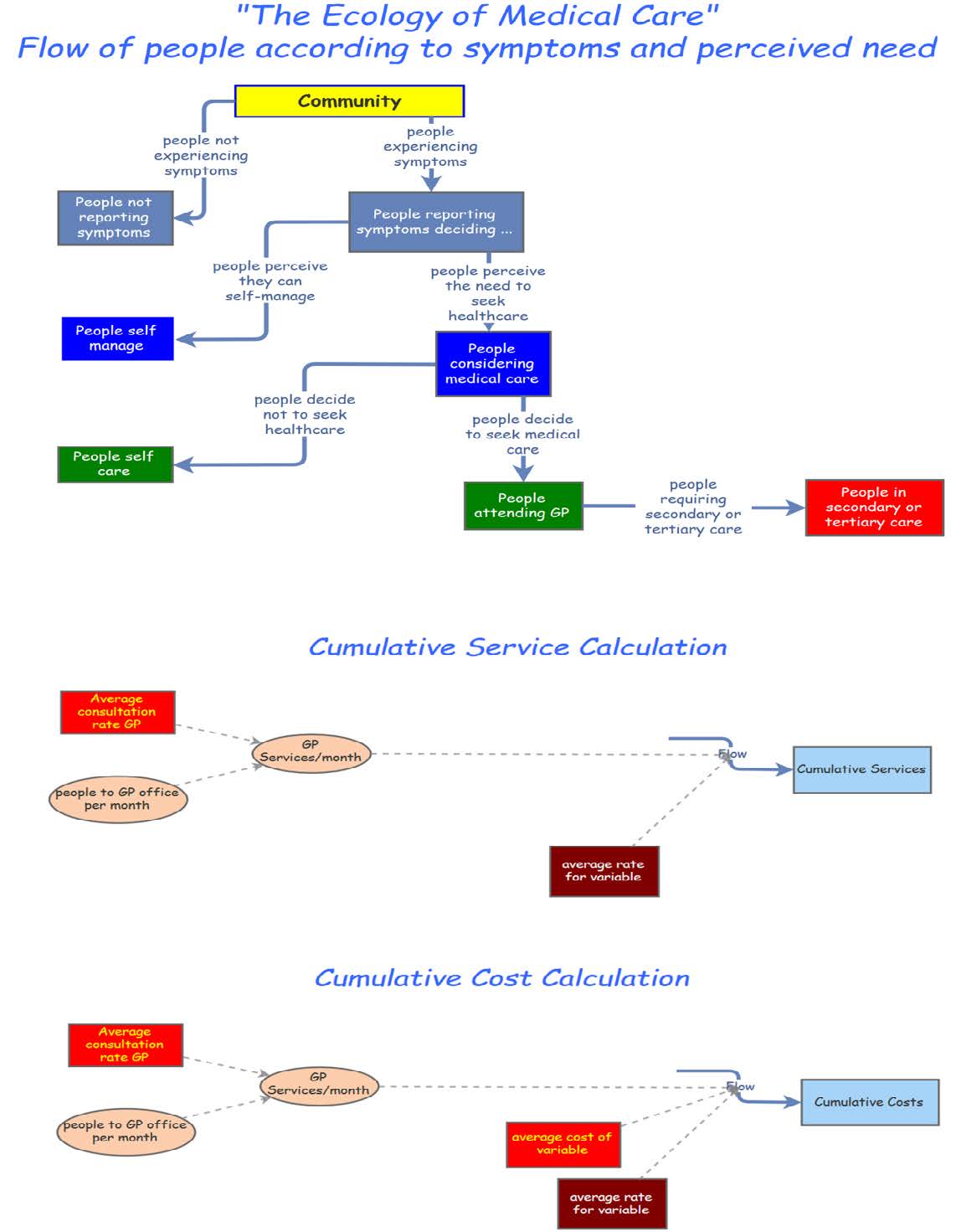
Fortmann-Roe S (2014) Insight Maker: A general-purpose tool for web-based modeling & simulation. Simulation Model Practice Theory 47: 28-45. doi: 10.1016/j.simpat.2014.03.013
|
| [7] |
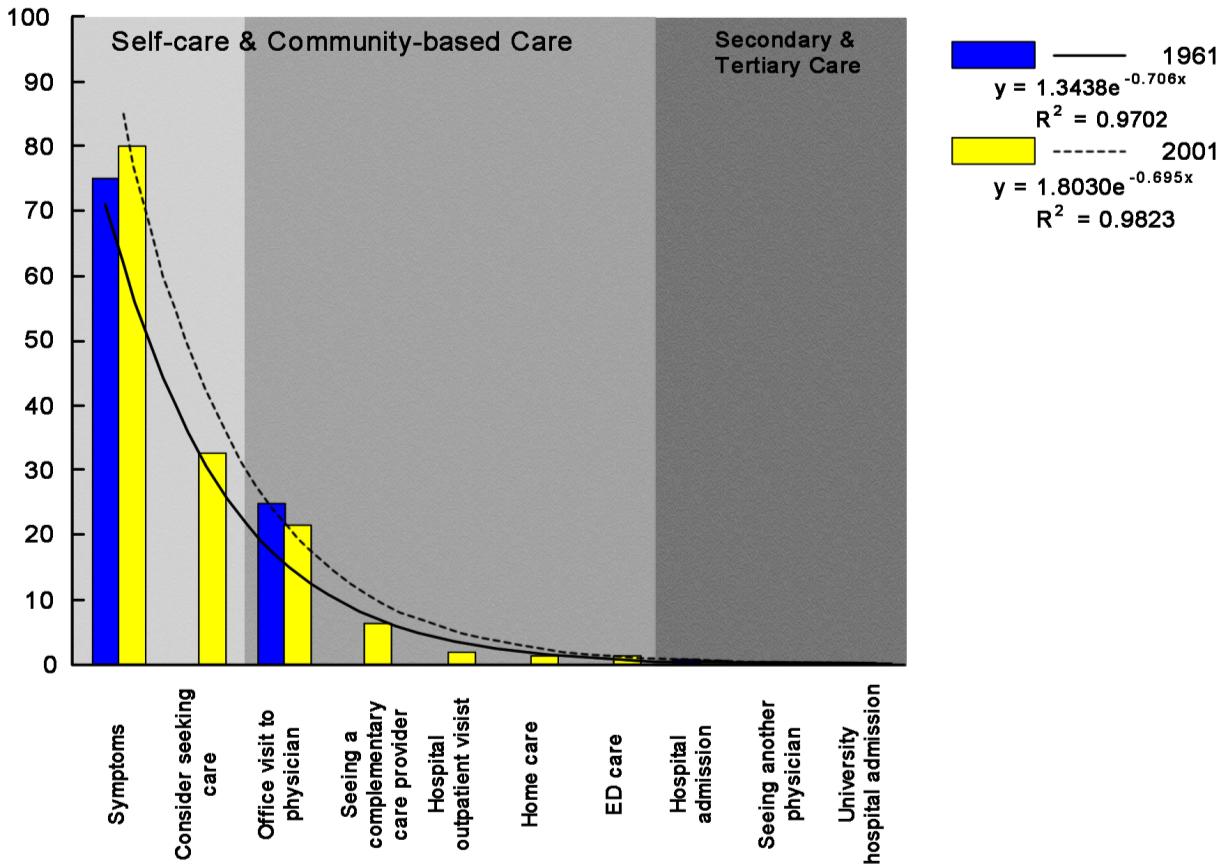
White K, Williams F, Greenberg B (1961) The Ecology of Medical Care. N Engl J Med 265: 885-892. doi: 10.1056/NEJM196111022651805
|
| [8] |
Green L, Fryer G, Yawn B, et al. (2001) The Ecology of Medical Care Revisited. N Engl J Med 344: 2021-2025. doi: 10.1056/NEJM200106283442611
|
| [9] |
Johansen ME, Kircher SM, Huerta TR (2016) Reexamining the Ecology of Medical Care. N Engl J Med 374: 495-496. doi: 10.1056/NEJMc1506109
|
| [10] | Sturmberg JP, O'Halloran DM, Martin CM (2014) Health Care Reform—The Need for a Complex Adaptive Systems Approach. In: Sturmberg JP, Martin CM, editors. Handbook of Systems and Complexity in Health. New York: Springer; p. 827-853. |
| [11] | Britt H, Miller GC, Henderson J, et al. (2013) General practice activity in Australia 2012–13. Sydney: 2013 Contract No.: General practice series no.33. |
| [12] | Australian Institute of Health and Welfare. (2014) Australian hospital statistics 2012–13. Canberra: Australian Institute of Health and Welfare, Cat. No. HSE 145. |
| [13] | Australian Institute of Health and Welfare. (2014) Australian hospital statistics 2012–13. Emergency department care. Canberra: Australian Institute of Health and Welfare, Cat. No. HSE 142. |
| [14] | Medicare Australia. (http://wwwmedicareaustraliagovau/cgi-bin/brokerexe?_PROGRAM=sasmbs_group_standard_reportsas&_SERVICE=default&DRILL=on&_DEBUG=0&GROUP=1&VAR=services&STAT=count&RPT_FMT=by+state&PTYPE=finyear&START_DT=201207&END_DT=201306). |
| [15] | Department of Health. http://wwwhumanservicesgovau/corporate/statistical-information-and-data/pharmaceutical-benefits-schedule-statistics/. |
| [16] |
Nissen SE (2015) Reforming the continuing medical education system. JAMA 313: 1813-1814. doi: 10.1001/jama.2015.4138
|
| [17] | Alper J, Geller A (2015) How modeling can inform strategies to improve population health: Workshop summary. National Academies of Sciences, Engineering, and Medicine. Washington, DC: The National Academies Press. |
| [18] |
Howie J, Heaney D, Maxwell M, et al. (1999) Quality at general practice consultations: cross sectional survey. Br Med J 319: 738-743. doi: 10.1136/bmj.319.7212.738
|
| [19] | Howie JGR, Porter AMD, Heaney DJ, et al. (1991) Long to short consultation ratio: a proxy measure of quality of care for general practice. Br J Gen Pract 41: 48-54. |
| [20] | Freeman G, Horder J, Howie J, et al. (2002) Evolving general practice consultation in Britain: issues of length and context. Br Med J 324: 820-822. |
| [21] |
Hart JT (1998) Expectations of health care: promoted, managed or shared? Health Expect 1: 3-13. doi: 10.1046/j.1369-6513.1998.00001.x
|
| [22] |
Hjortdahl P, Borchgrevink CF (1991) Continuity of care—influence of general practitioners' knowledge about their patients on use of resources in consultations. Br Med J 303: 1181-1184. doi: 10.1136/bmj.303.6811.1181
|
| [23] |
Hjortdahl P (1992) The Influence of General Practitioners' Knowledge about their Patients on the Clinical Decision-Making Process. Scand J Prim Health Care 10: 290-294. doi: 10.3109/02813439209014076
|
| [24] |
Reeve J, Blakeman T, Freeman G, et al. (2013) Generalist solutions to complex problems: generating practice-based evidence—the example of managing multi-morbidity. BMC Family Practice 14: 112. doi: 10.1186/1471-2296-14-112
|
| [25] |
Stange KC, Ferrer RL (2009) The Paradox of Primary Care. Ann Fam Med 7: 293-299. doi: 10.1370/afm.1023
|
| [26] | Martin CM, Grady D, Deaconking S, et al. (2014) Complex adaptive chronic care—typologies of patient journey: a case study. J Eval Clin Pract 17: 520-524. |
| [27] | Sturmberg JP, O’Halloran DM, Martin CM (2010) People at the centre of complex adaptive health systems reform. Med J Aust 193: 474-478. |
| [28] | Heifetz R (1994) Leadership Without Easy Answers. Cambridge, Ma: Harvard University Press. |
Figures(3) / Tables(2)

Joachim P Sturmberg, Geoff M McDonnell. How Modelling could Contribute to Reforming Primary Care—Tweaking “the Ecology of Medical Care” in Australia[J]. AIMS Medical Science, 2016, 3(3): 298-311. doi: 10.3934/medsci.2016.3.298







 DownLoad:
DownLoad: